













Thorax Preview Case 1
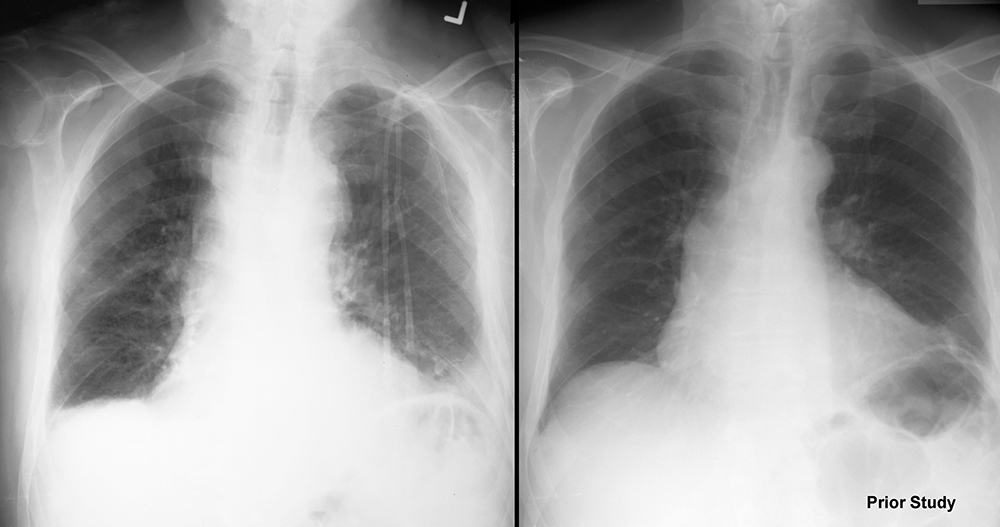
68 year old patient who had a central line placed and had imaging performed.
Question 1:
a) What is a central line?
A central line (central venous line or CVL for short) is a thin piece of plastic tubing that is placed into a large vein and threaded inward until the tip is in a 'central' position, ideally in the superior vena cava.
b) What are large veins that are relatively easy to access for placement of a CVL?
The commonest veins that are used are the femoral vein, the subclavian vein and the internal jugular vein.
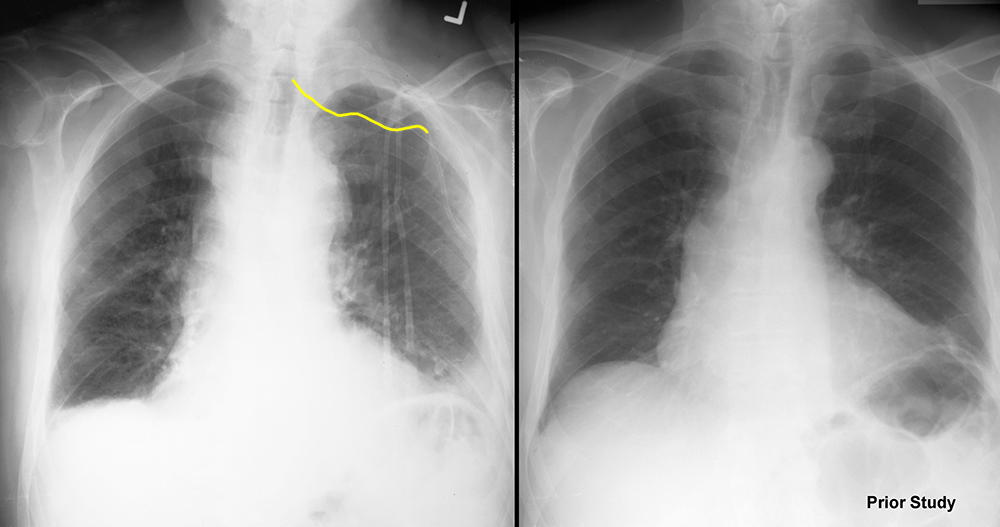
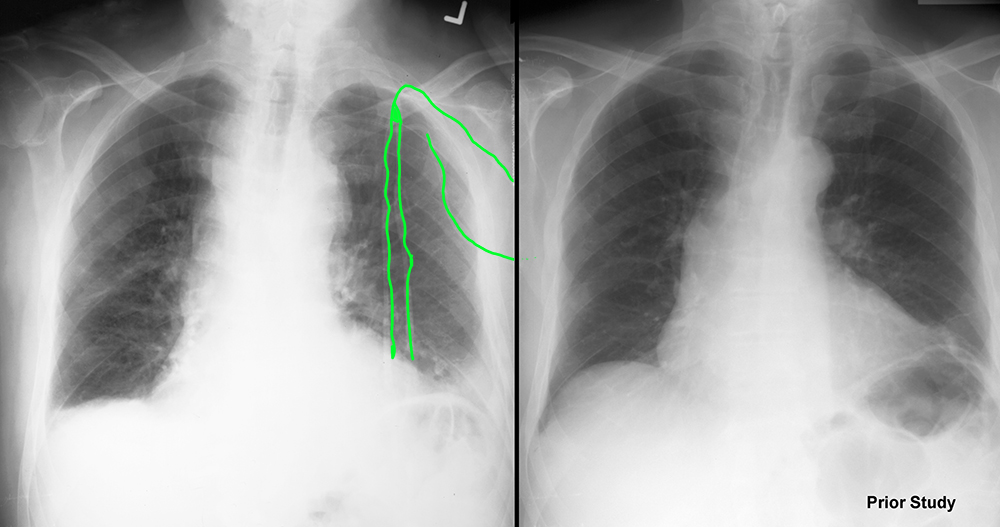
c) Which vein was likely used in this case? If you are having trouble seeing the CVL, use the links below (CVL internal and CVL external) to see the parts of the catheter that are OUSIDE the patient and INSIDE.
The left subclavian vein, based on the location of the portion of the CVL labeled as internal.
d) Do you think the CVL in this case is directed appropriately toward the superior vena cava?
NO! The internal course indicated does not make sense for the left subclavian, and the connecting vessels that drain into the superior vena cava.

Thorax Preview Case 1
These diagrams show the approximate course of a right subclavian CVL (recall that our patient has a CVL on the left, not the right). The diagrams were obtained from a chest CT dataset. How are the patient's arms positioned for a chest CT and how would that affect the position of the clavicle?
Question 2:
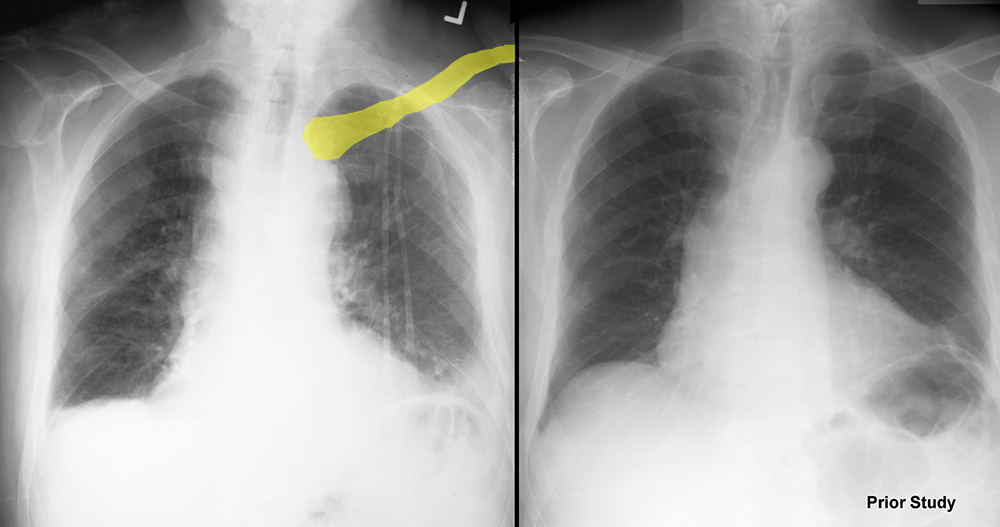
a) Where would you expect a right subclavian CVL to be located relative to the clavicle?
The point of entry of the catheter into the vein is usually inferior to or just deep to the clavicle, but the course may arch upward running parallel to the upper margin of the clavicle. The position of the subclavian vein relative to the clavicle is variable from patient to patient, but the vessel usually runs parallel to the bone, either superior, deep to, or slightly inferior on radiography.
b) Is a chest radiograph necessary after placement of a CVL?
Yes! It is very important to be sure that the CVL is going where it should be, and that there are no complications from placement. A chest radiograph is a great way to answer these questions.
c) What are complications of placement of a CVL?
One possible complication is bleeding from traversing the tissues from skin to vessel. Another complication is pneumothorax, if the needle used is placed too deeply and pierces the lung. Another complication is incorrect placement into the wrong vessel.
Thorax Preview Case 1
For a chest CT, the patient's arms are usually over their head, to make the upper chest more cylindrical in cross section (and reduce artifacts in the images), and this will result in slightly higher position of the clavicles than for a patient lying supine in bed with their arms at their sides.
Question 3:
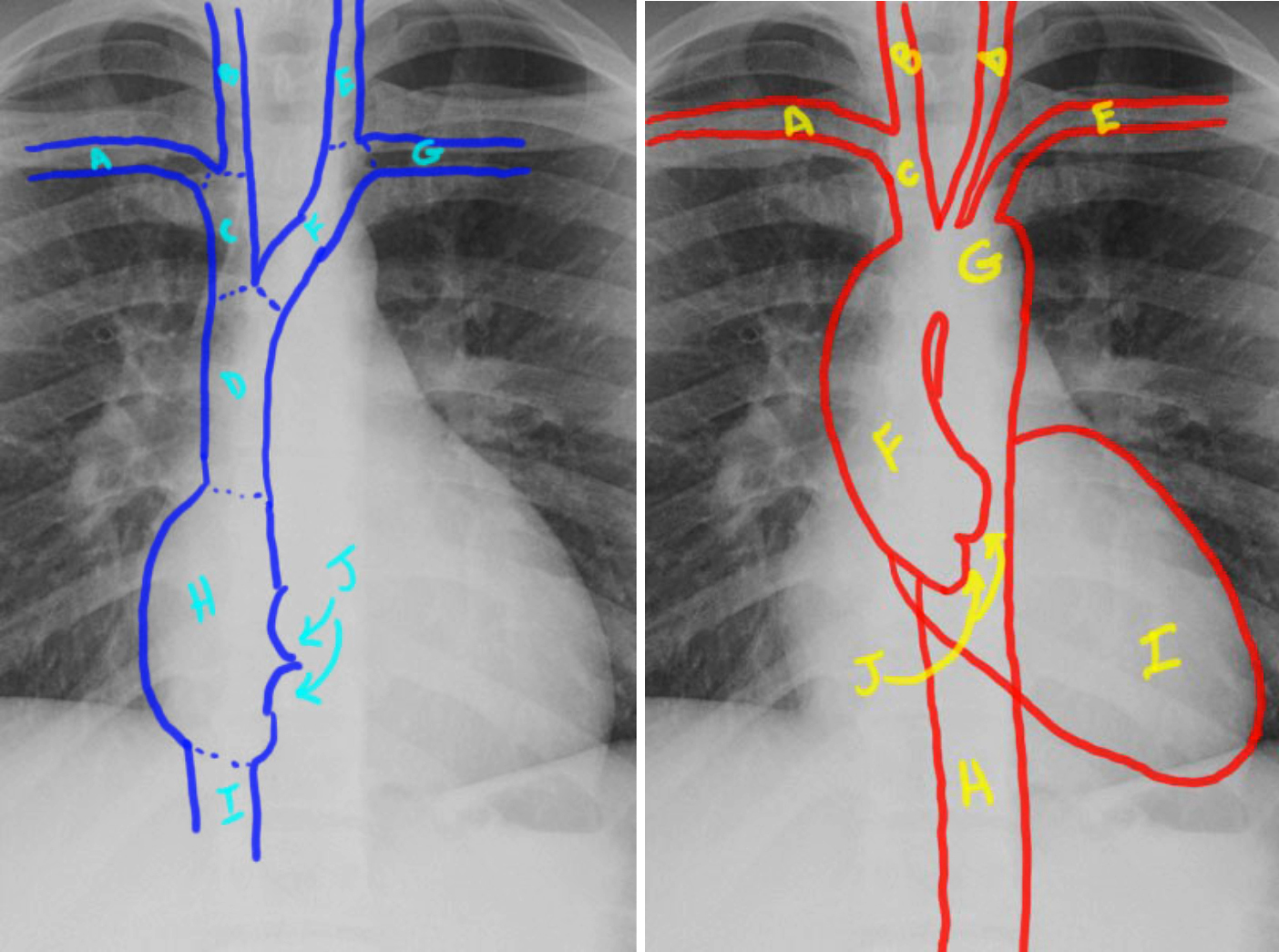
a) This image shows the major arterial and venous structures visible on chest radiography, which were reviewed on the previous page. Which vessels are important to identify for the case on the first page?
For a left subclavian CVL, the left subclavian (G), left brachiocephalic (F) and superior vena cava (D) are important to locate.
b) What abnormal vessel might the CVL on the first page be entering, based on this diagram?
Since the CVL is pointing upward and toward the midline, rather than downward, it might be entering the left internal jugular vein (E).
Thorax Preview Case 1
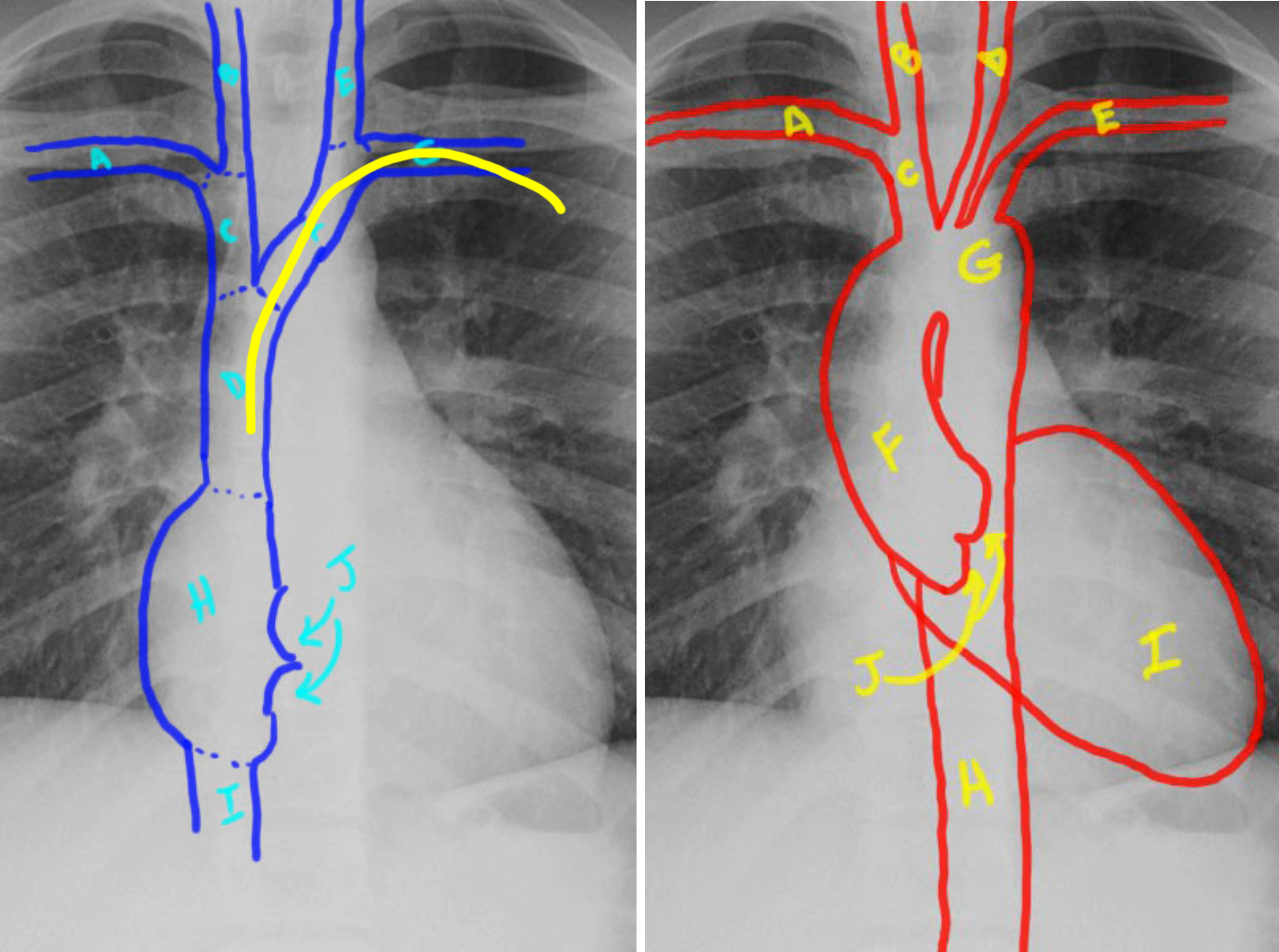
This is the same image shown on the first page, the patient with an attempted left subclavian CVL placement.
Question 4:
a) Is there any other possibility for this catheter course other than entry into the internal jugular vein?
Since the catheter is going medially and superiorly (rather than following the expected course of the left brachiocephalic vein), it could be entering a small venous tributary, such as the anterior jugular vein. Alternatively, it could be extravascular in location.
b) What would you do next?
There are several possibilities. It would make sense to have interventional radiology try injecting some contrast into the catheter to see if it seems to be in a small vessel. Or CT would also make sense, to see the course of the catheter better.




