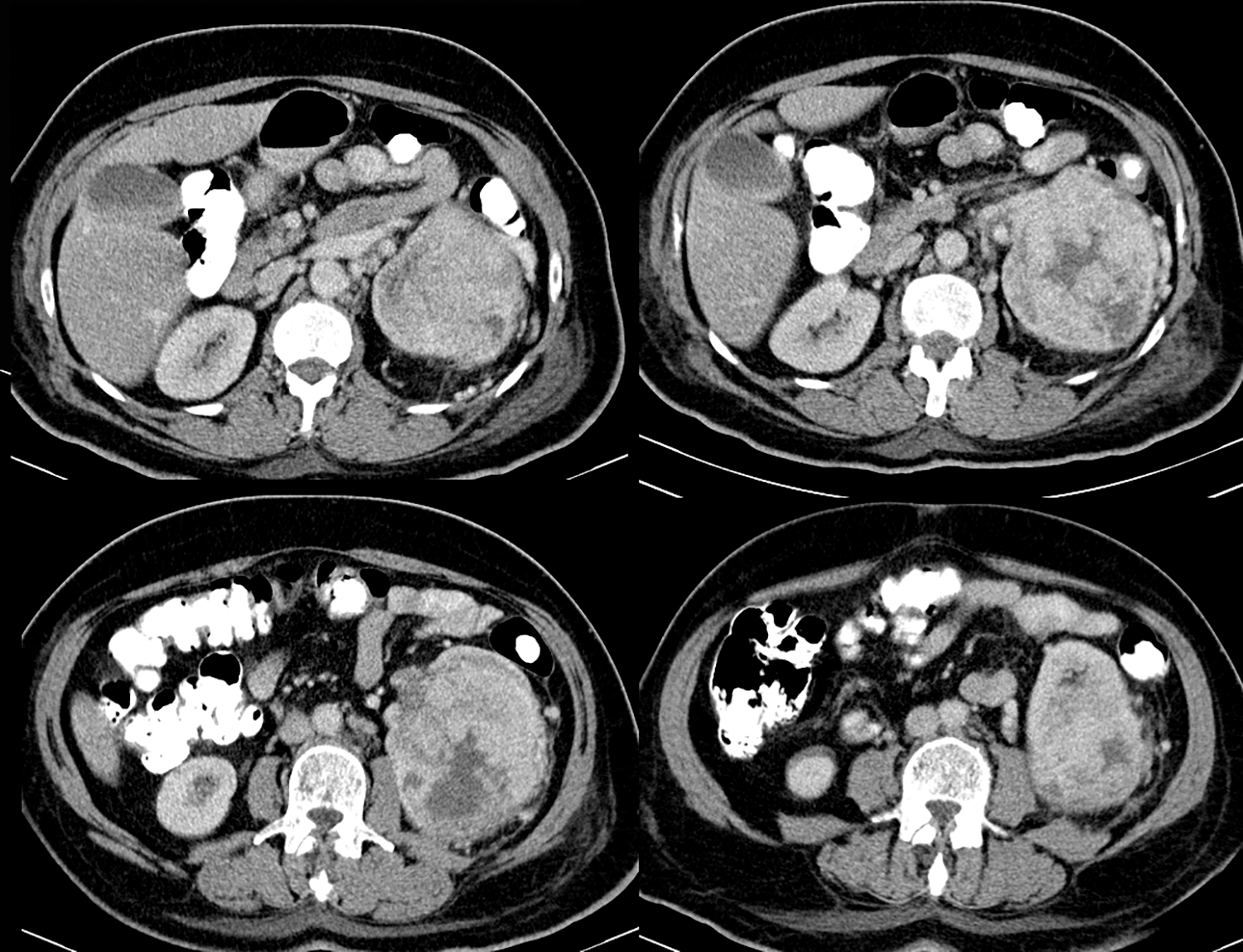
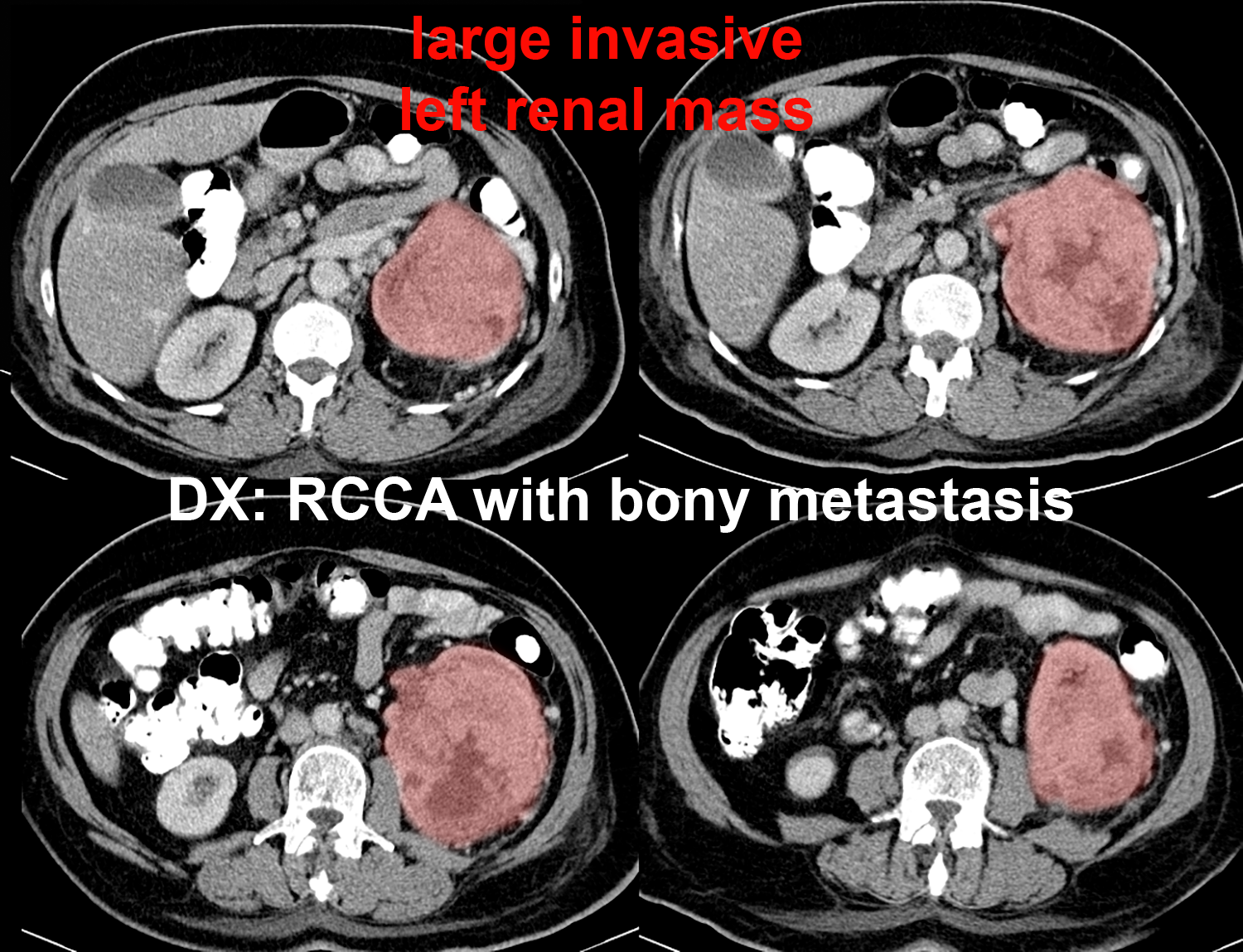
Imaging for Staging of RCCA
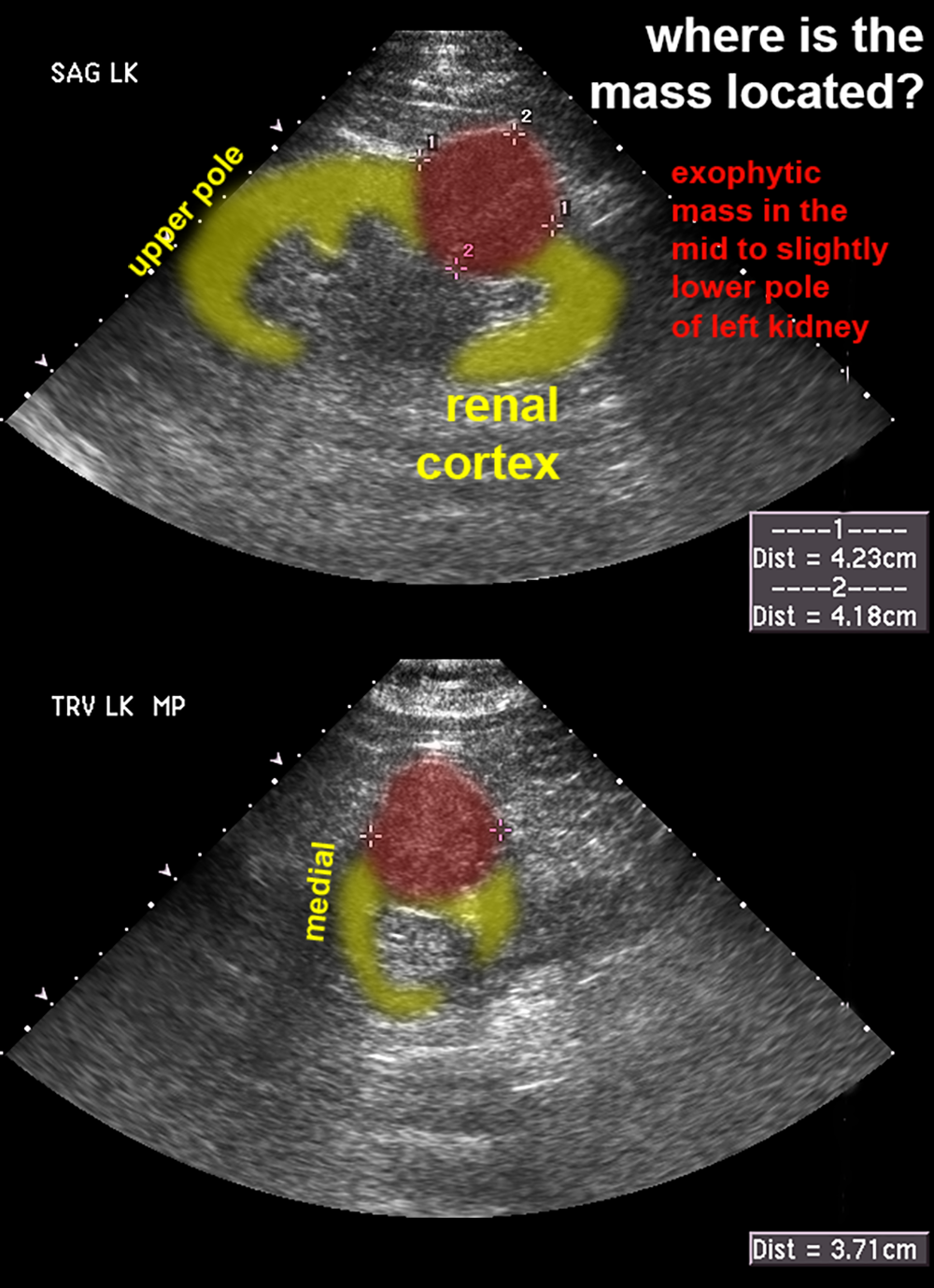
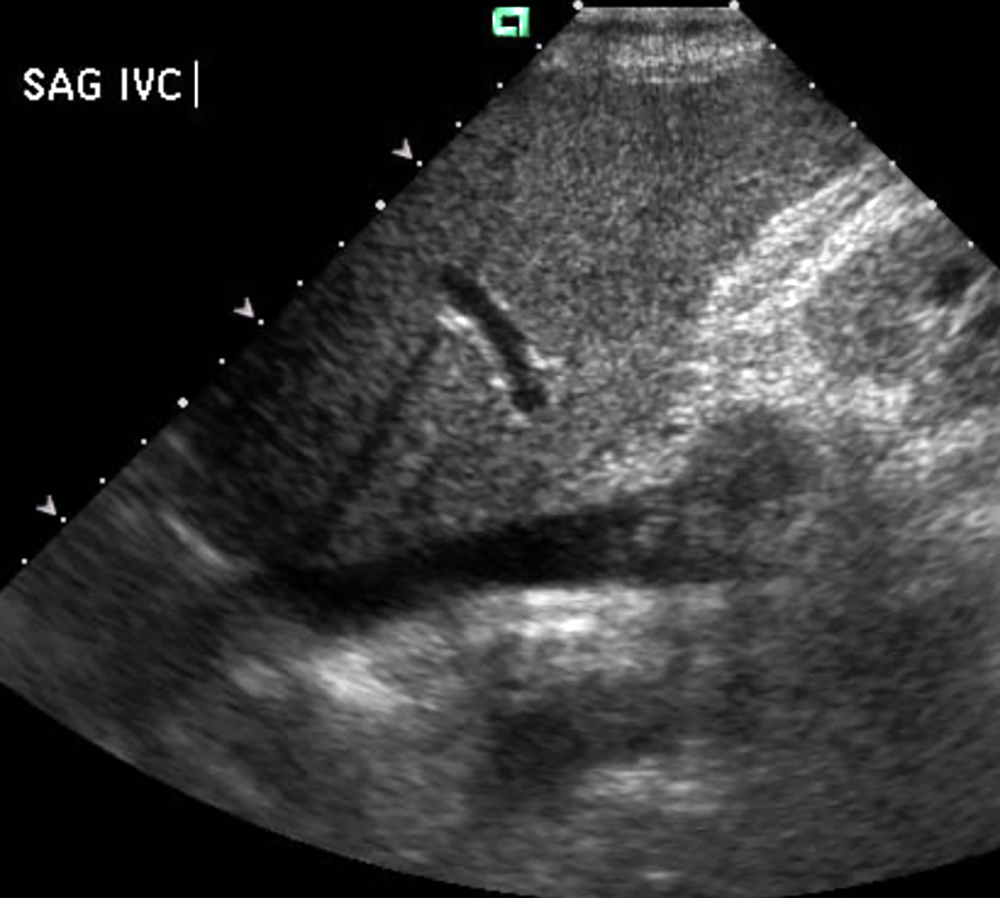
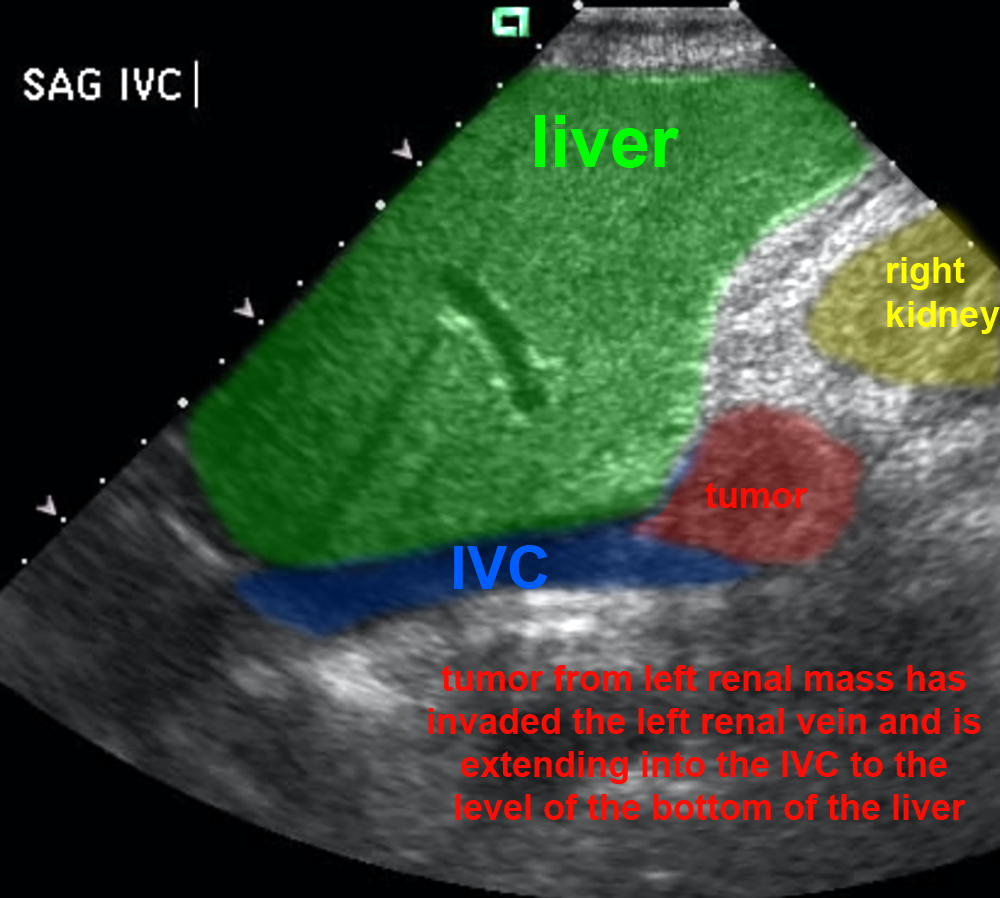
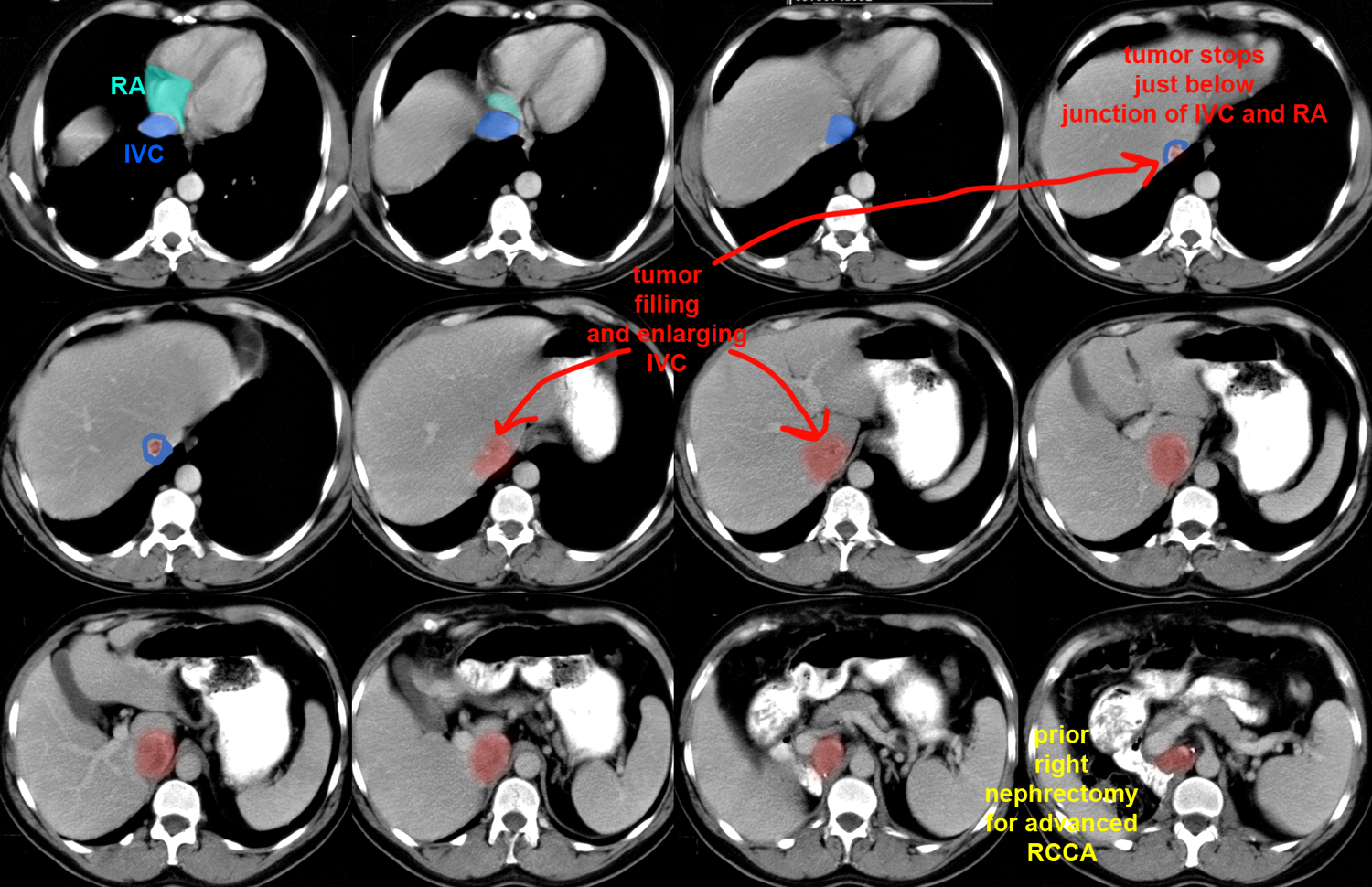
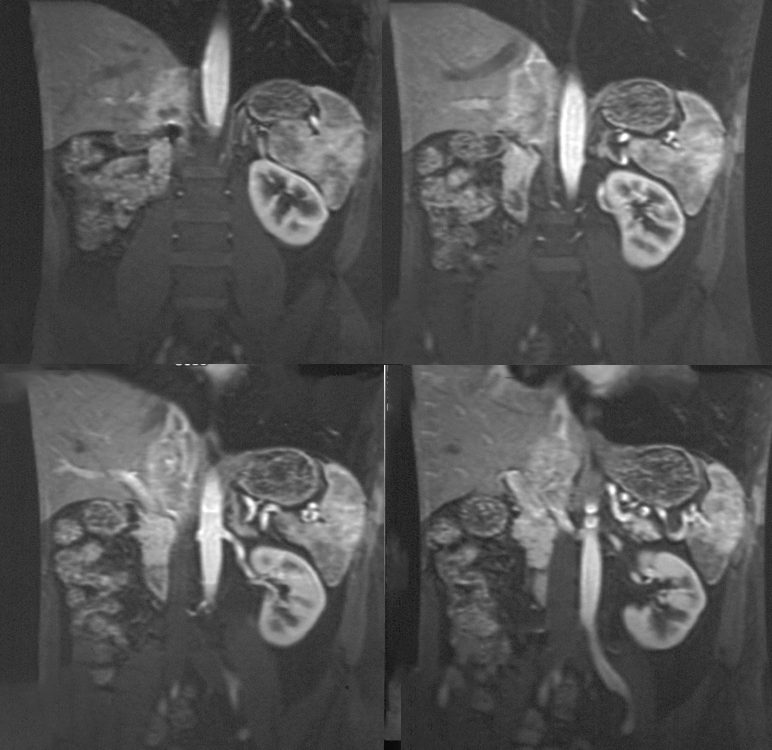
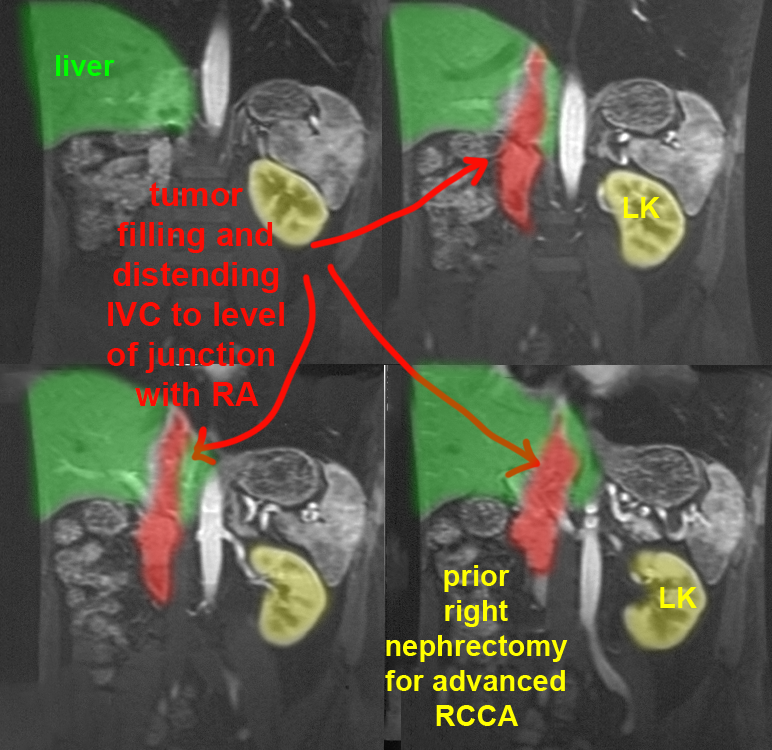
Renal cell carcinoma (RCCA) has many unique features in terms of spread that are relevant for staging. Imaging often plays a crucial role in determining such features as size, invasion beyond the renal capsule, beyond Gerota's fascia, or into adjacent organs and distant metastatic sites. One important aspect of RCCA staging relates to its propensity for direct invasion of veins draining the kidney. Detection of this can be with ultrasound, CT, or MR, and the level to which the tumor has spread is an important staging feature--invasion of the renal vein, IVC or right atrium all have important prognostic implications and can be detected with imaging. Invasion of the IVC has been reported in up to 10% of patients with RCCA.
Further Explanation:
Imaging for Staging of RCCA
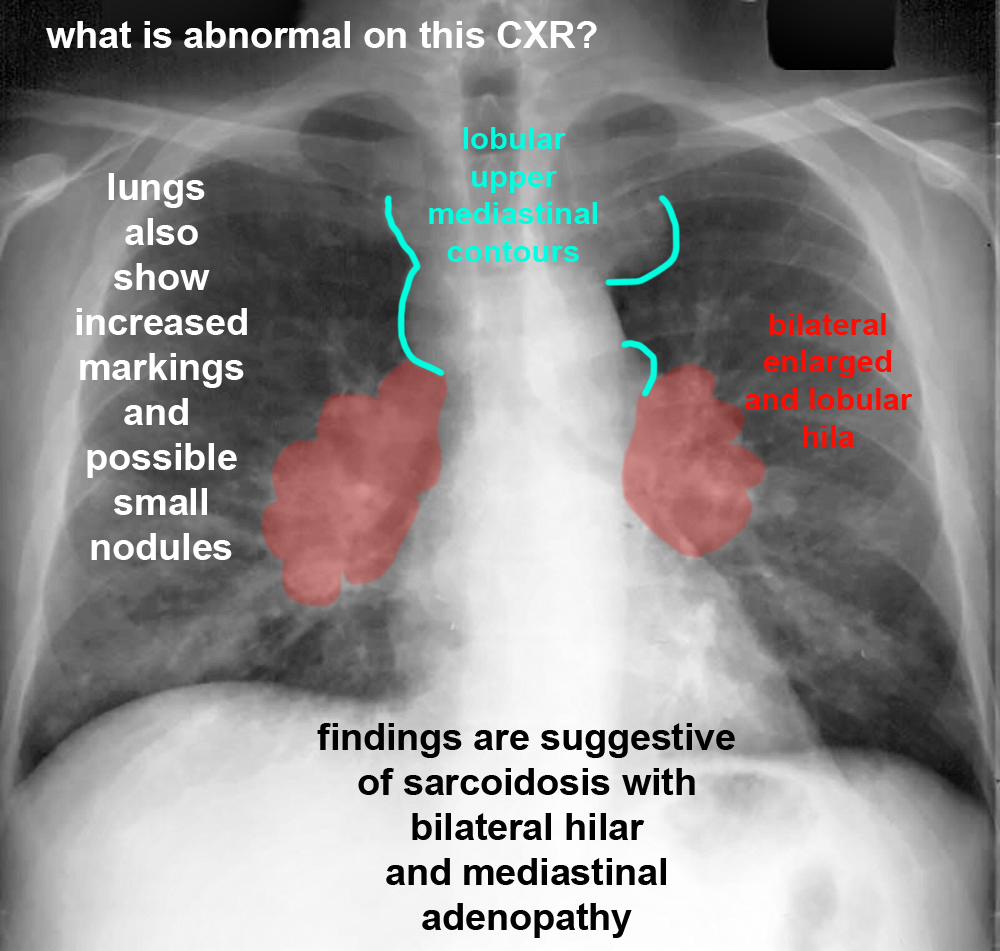
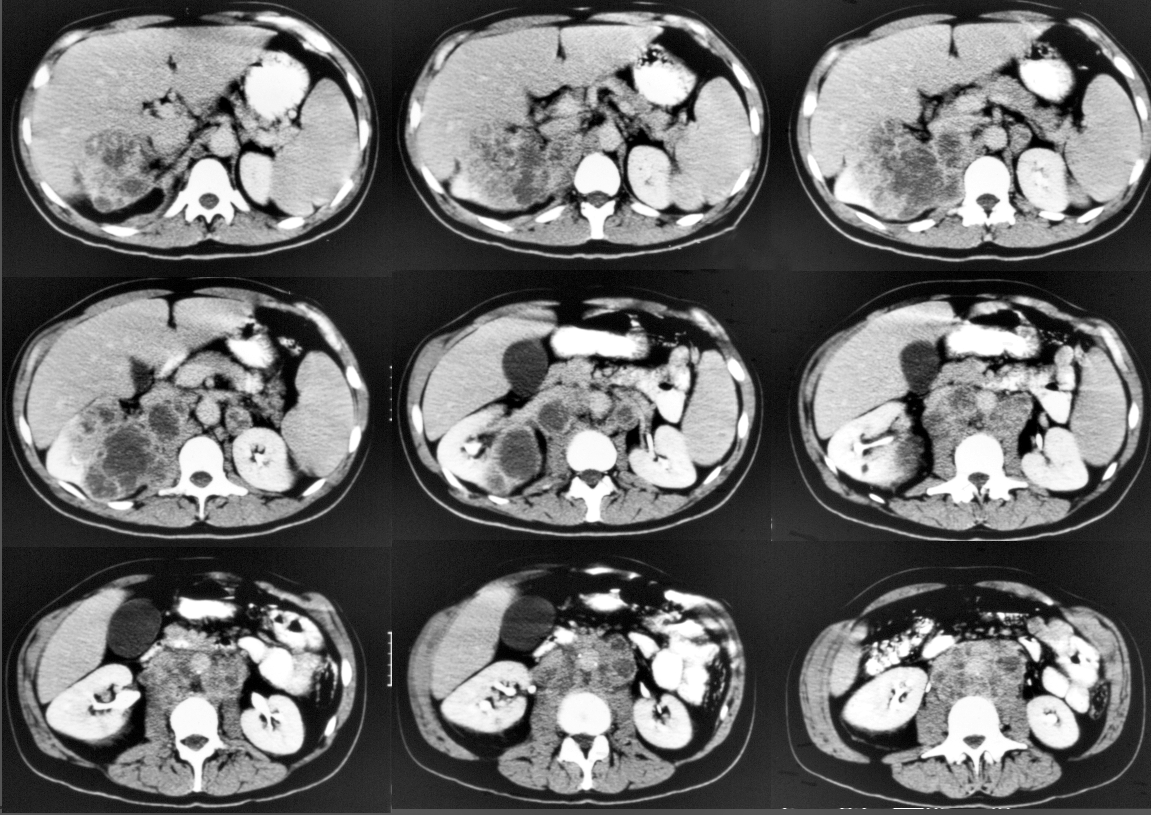
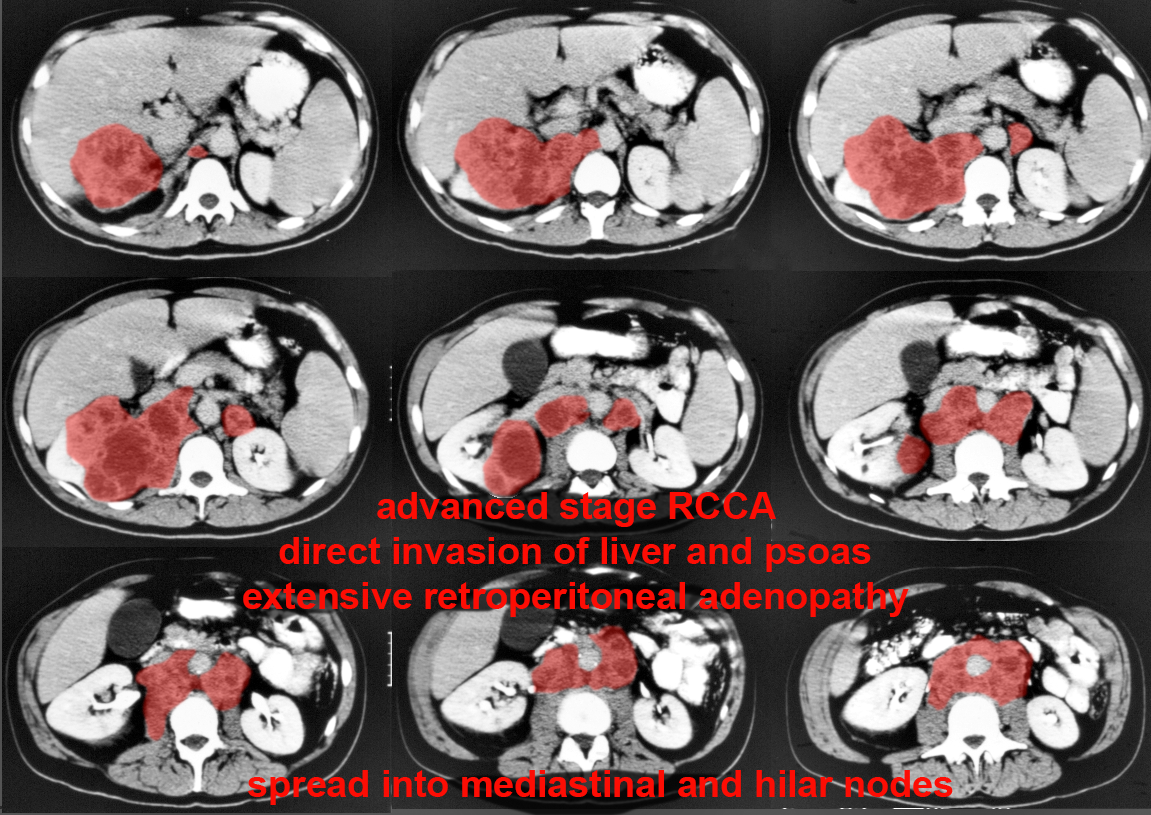
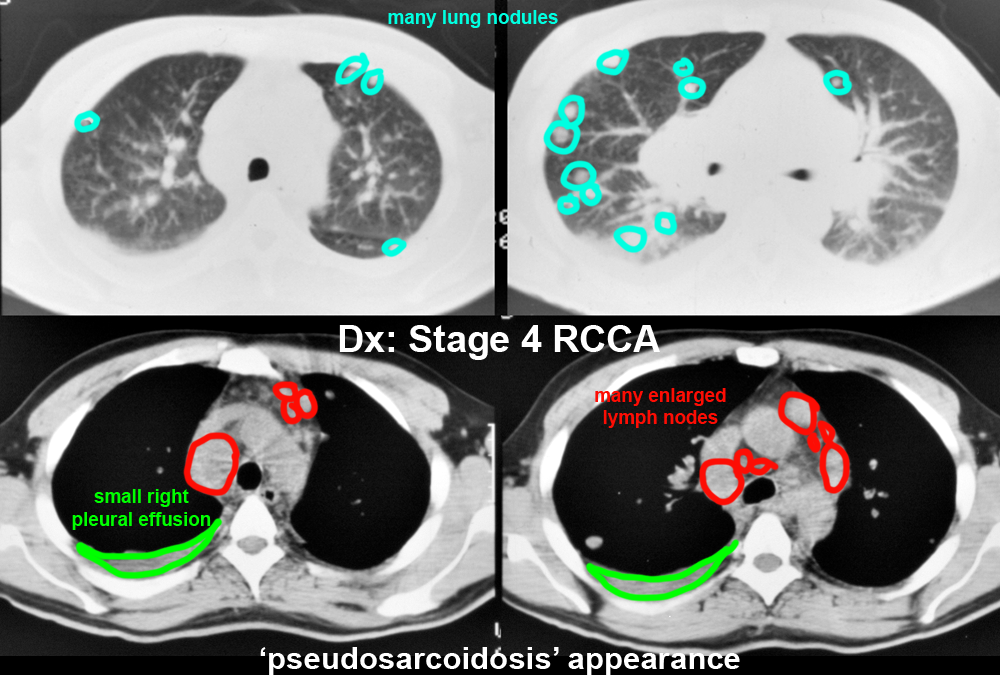
The commonest sites of metastatic spread of RCCA, in order of frequency, are lung, lymph nodes, bone and liver, but many other sites of metastases have been reported. In terms of nodal spread, RCCA can travel up from the retroperitoneum into the mediastinum, giving an unusual appearance that has been called 'pseudosarcoidosis'. This page demonstrates the findings of a patient with this condition. Pseudosarcoidosis is most often due to metastatic spread from either RCCA or testicular tumors.
Further Explanation:
Imaging for Staging of RCCA
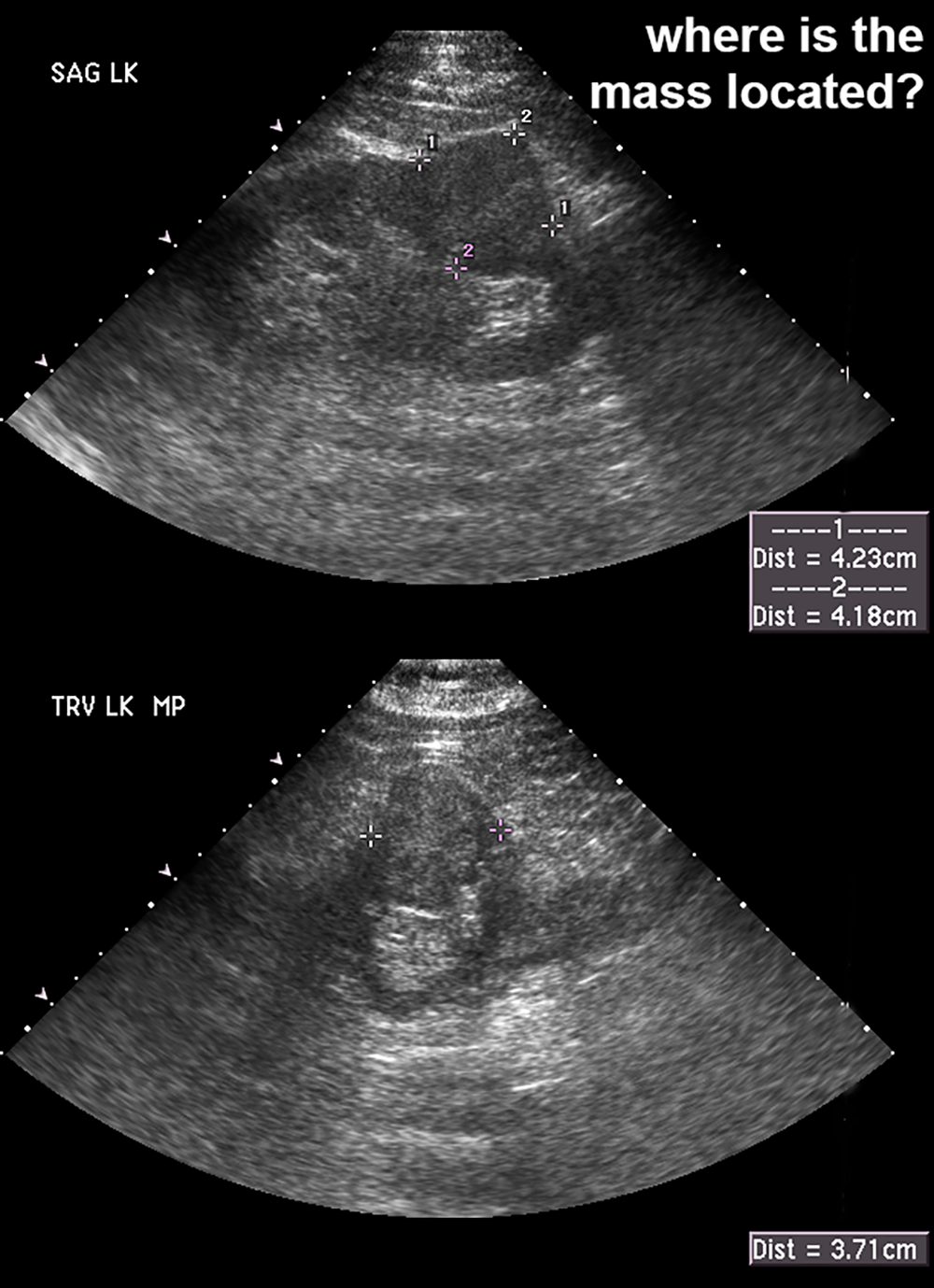
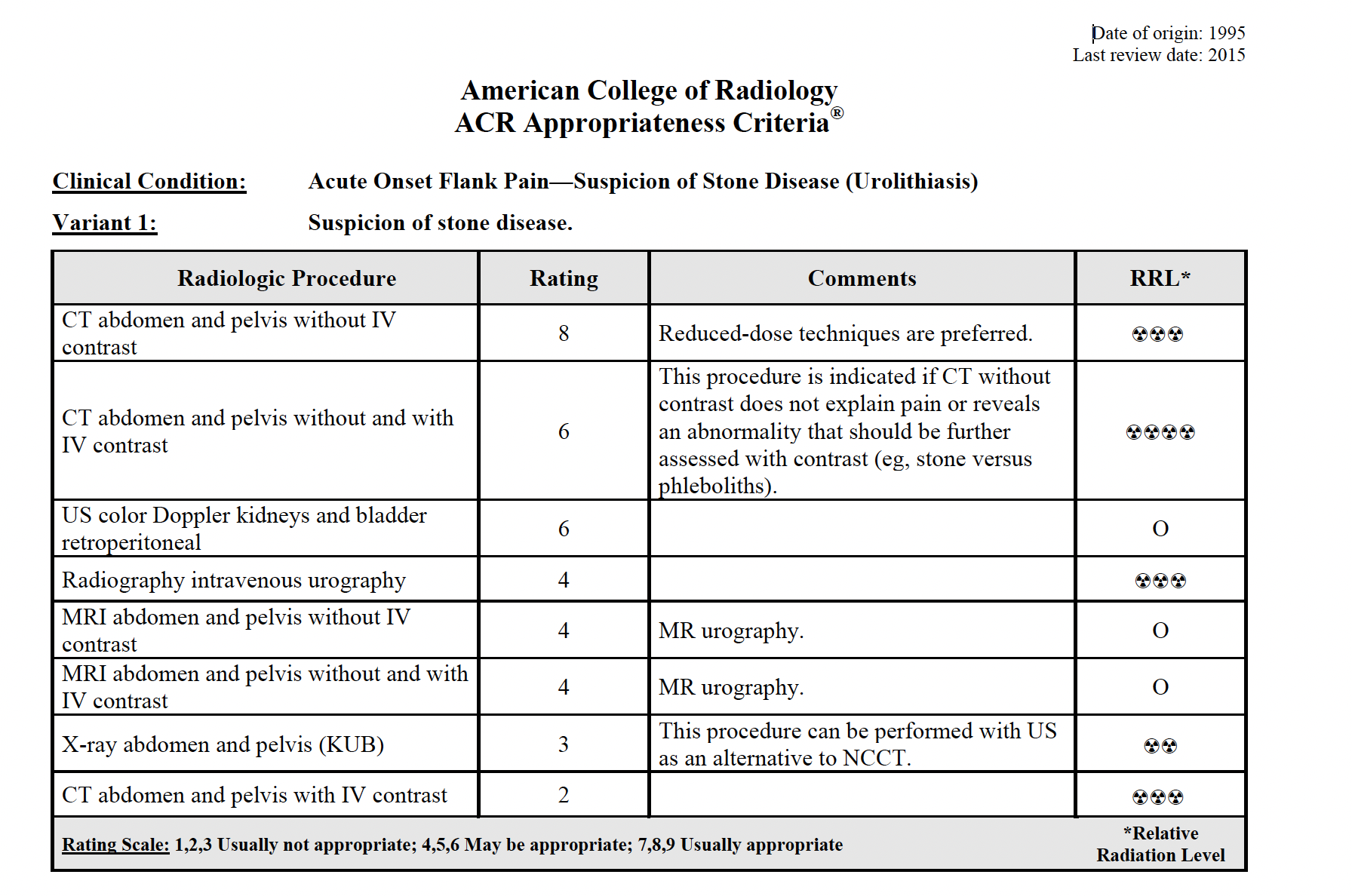
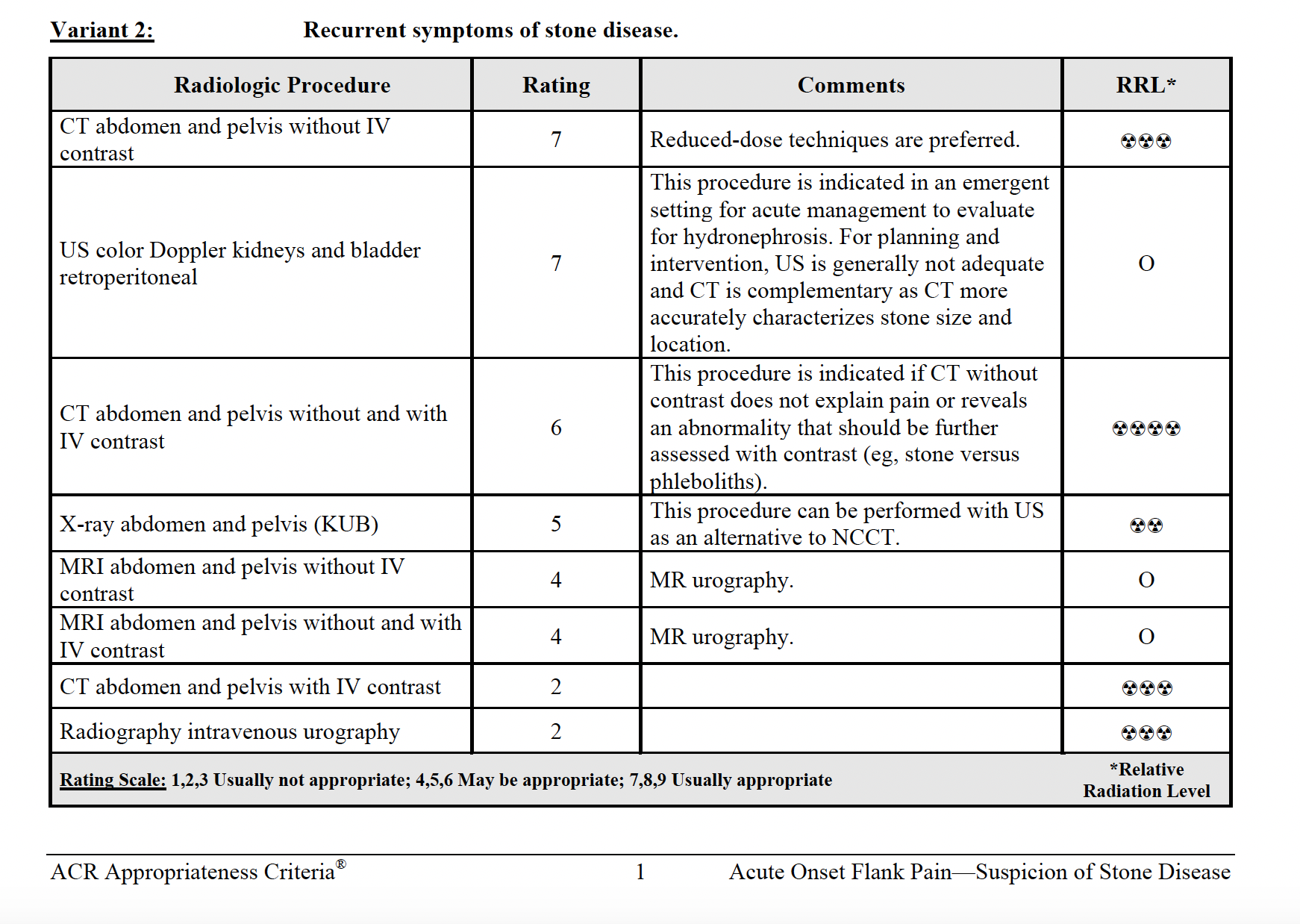
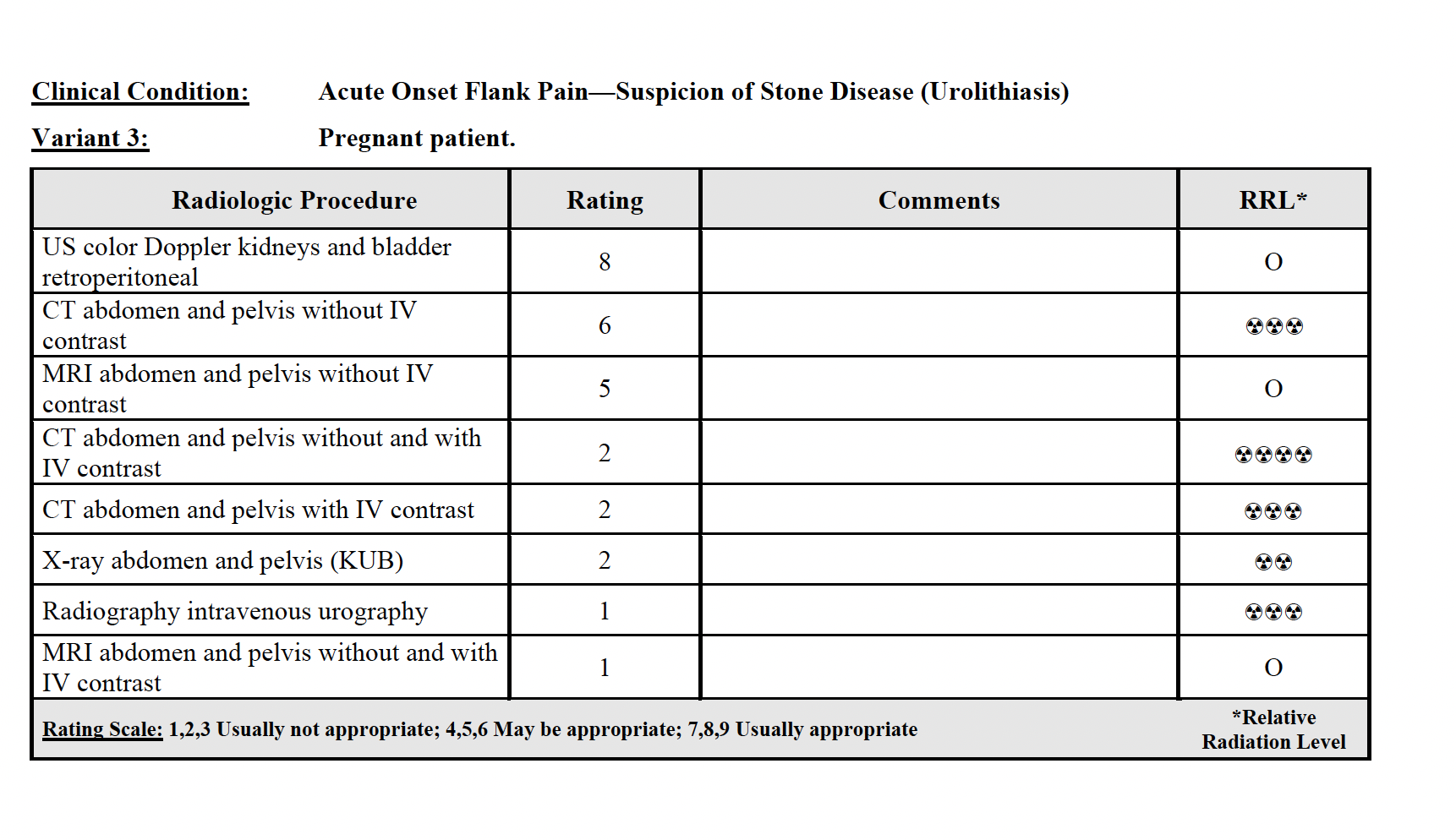
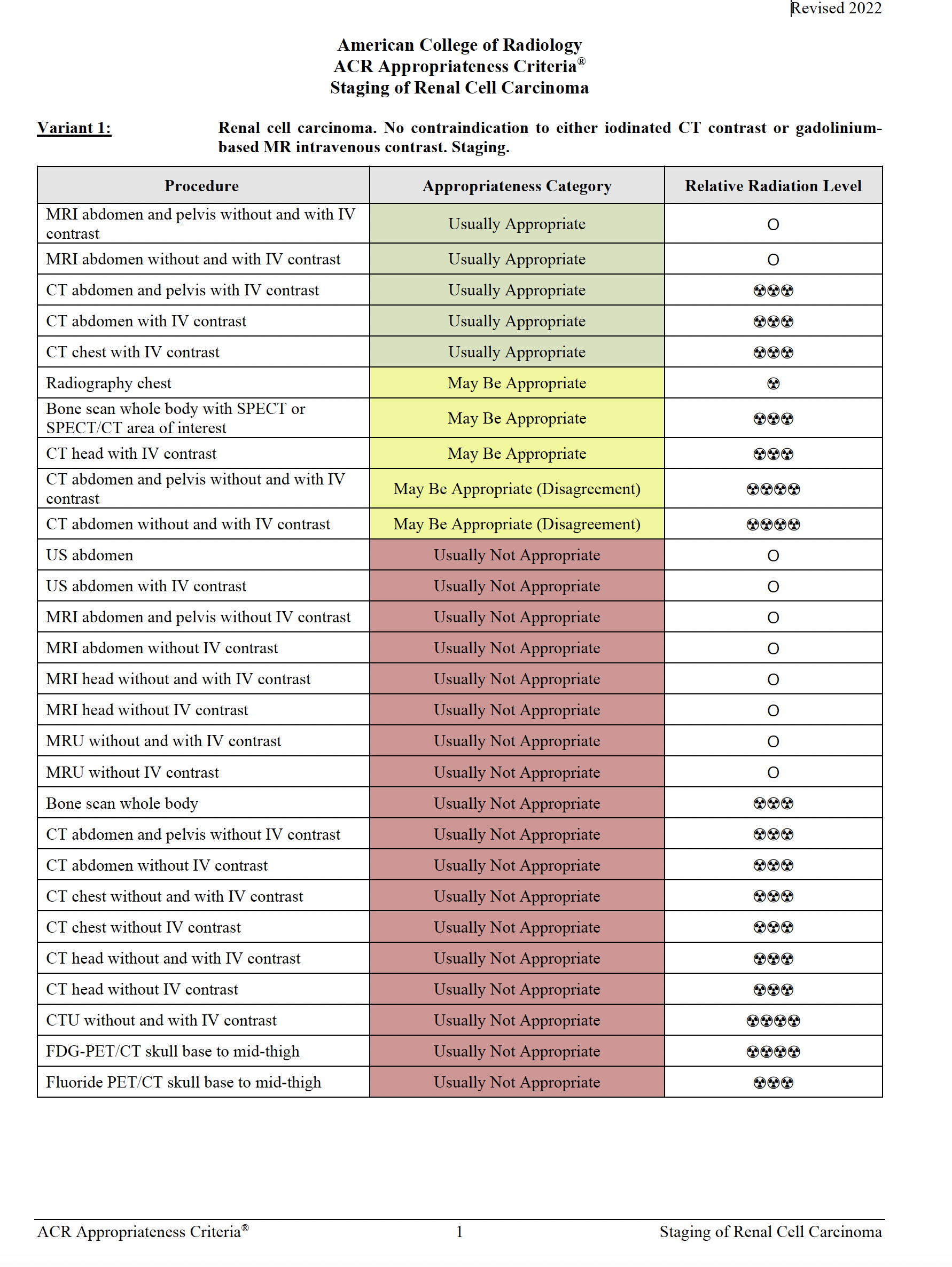
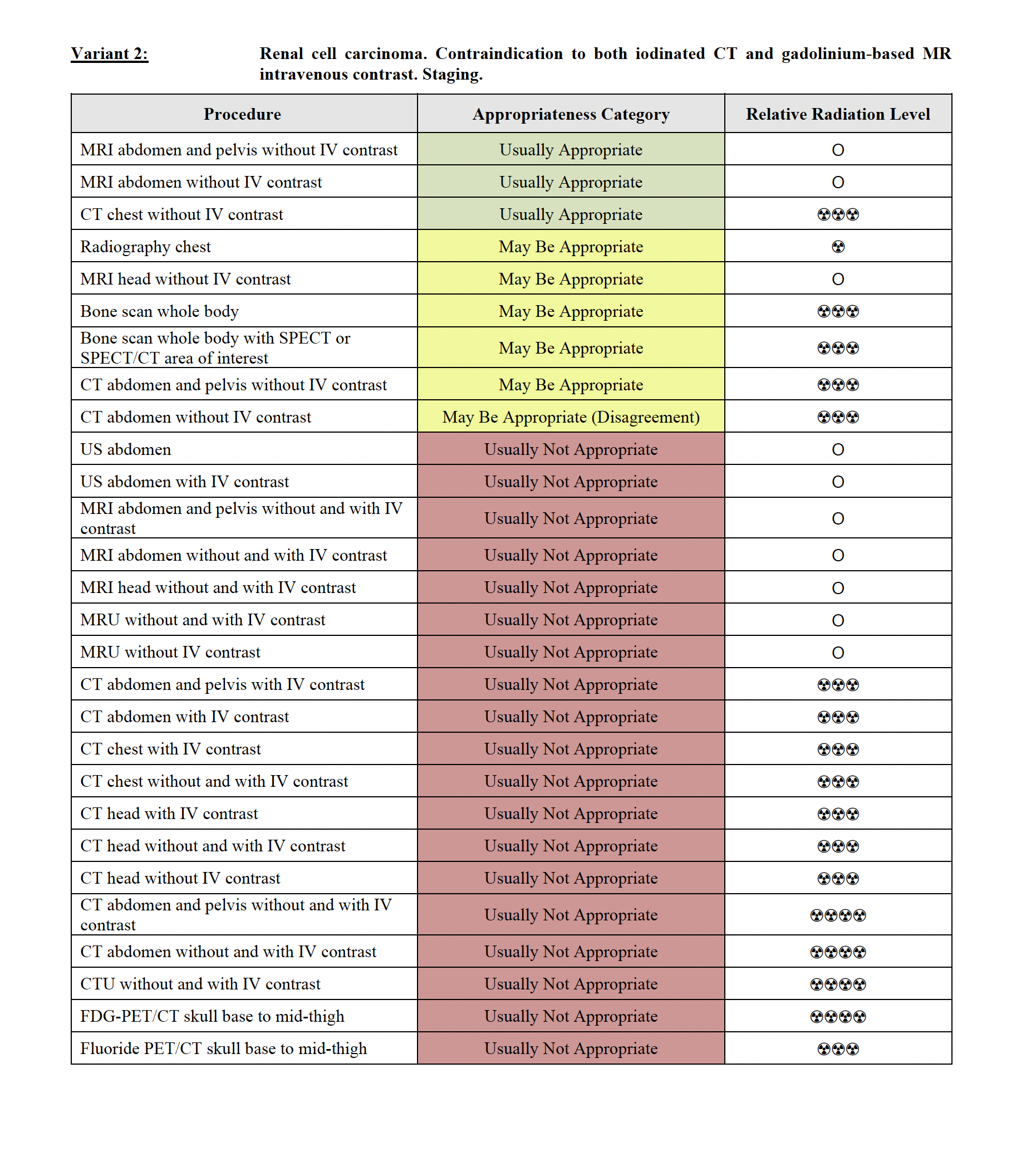
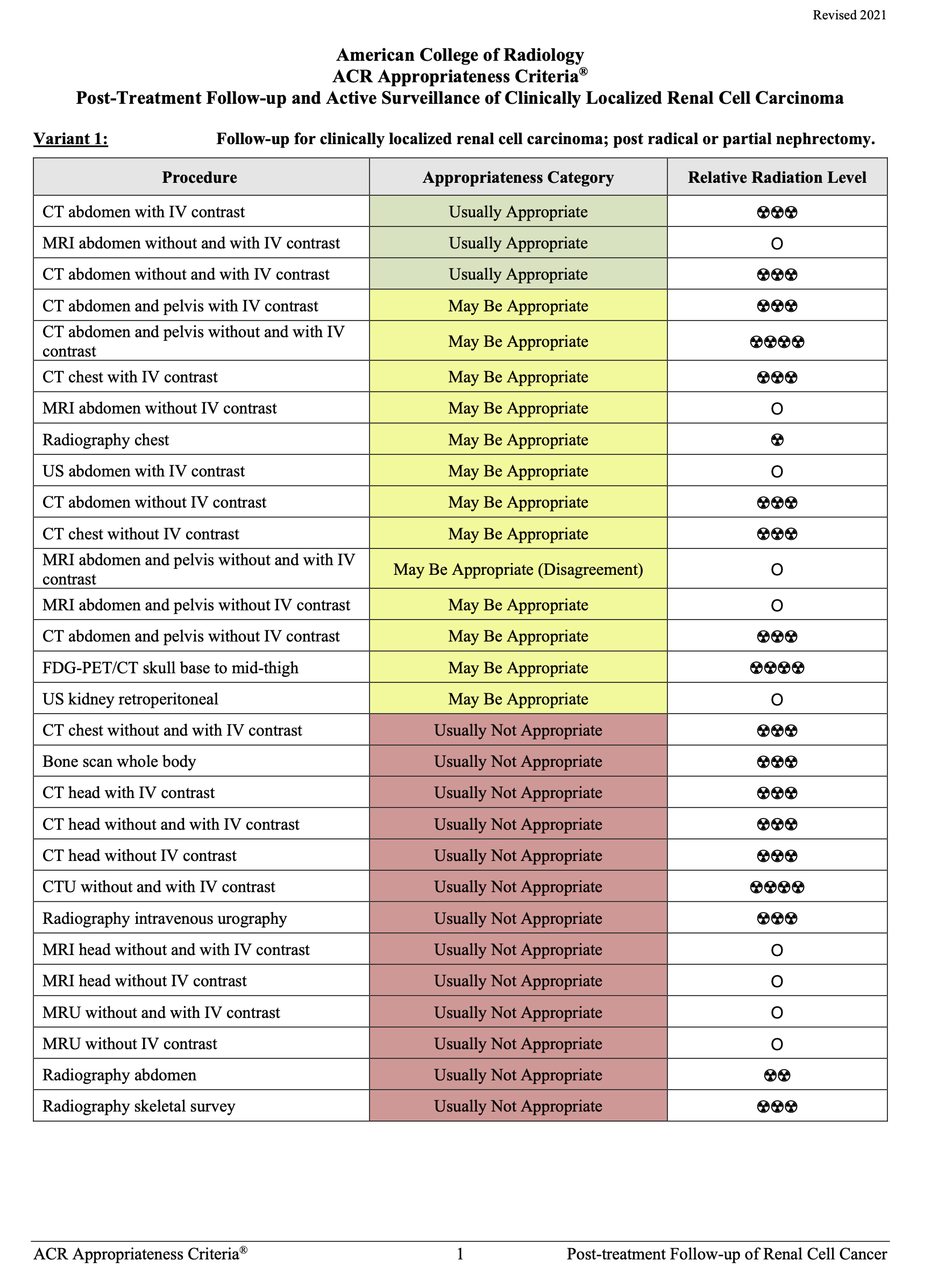
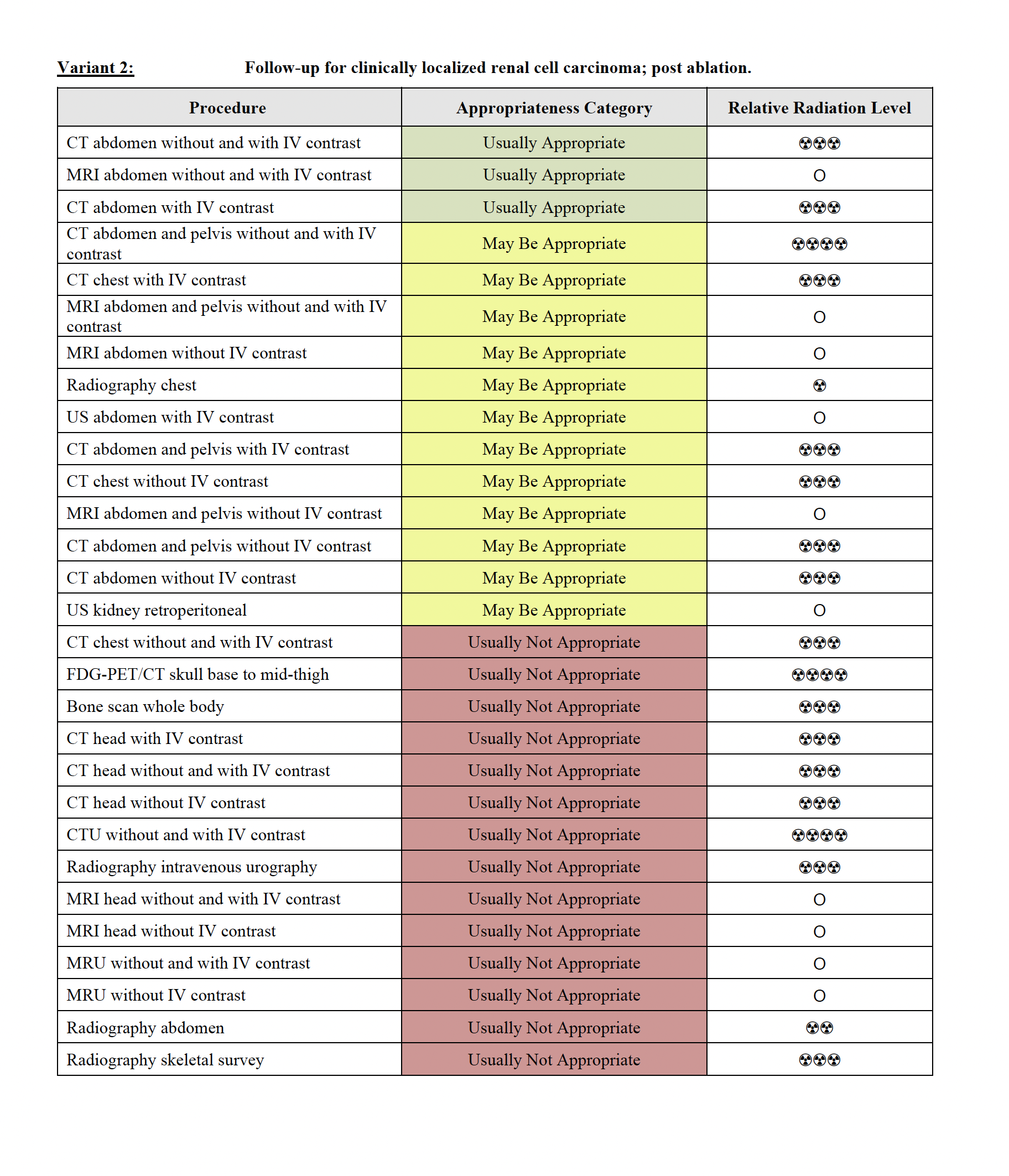
Because the analysis of cystic renal masses is so complex, a grading system has been developed, initially published by MA Bosniak in 1986, with many updates since that time, most recently in 2019. Many of the changes have reflected availability of newer imaging modalities as well as changes in treatment options. The system uses five different categories (I, II, IIF, III and IV) and respective maligancy rates in a recent meta-analysis were 3%, 6%, 7%, 55% and 91%. Category 1 is a simple cyst, while category II allows a few complicating features (hairline thin septa, fine calcifications, homogeneous hyperdensity without enhancement). Both Category I and II are considered benign, with no indication for further imaging or followup. Category IIF requires followup, with more septa, minimal enhancement, or more calcifications. Category III is a complicated cystic mass with more septa, more enhancement and more irregularity, while category IV shows a likely malignant mass with cystic components. As new imaging methods are developed to better characterize lesions, this system will likely be further modified. The ACR Appropriateness Criteria are another helpful resource for imaging many renal problems, and in staging a presumed or diagnosed RCCA. This page includes several of the recommendations from ACR for various renal scenarios. This resource can be accessed without a password, with all information freely available, including useful documents such as patient information sheets for various types of imaging studies, and narrative explanations for the recommendations with current references.
Further Explanation:
Imaging for Staging of RCCA
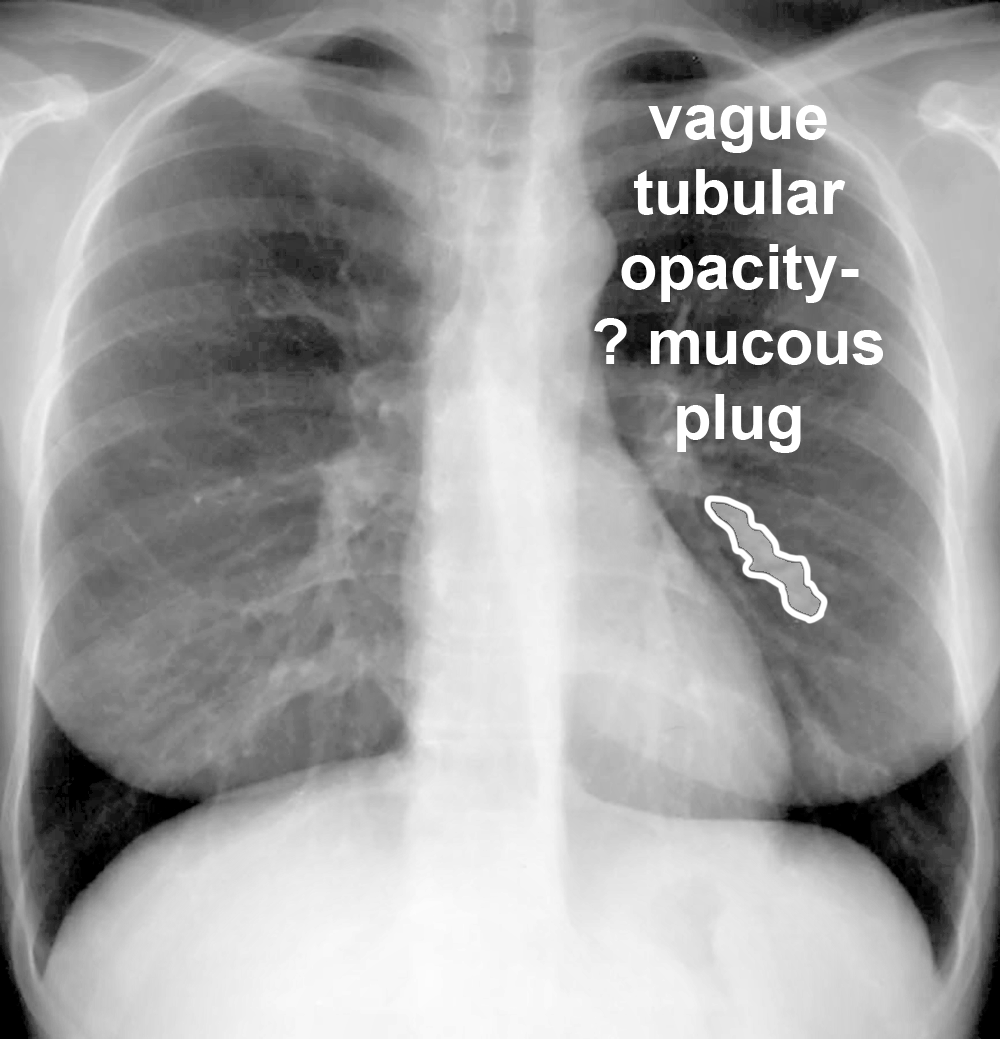
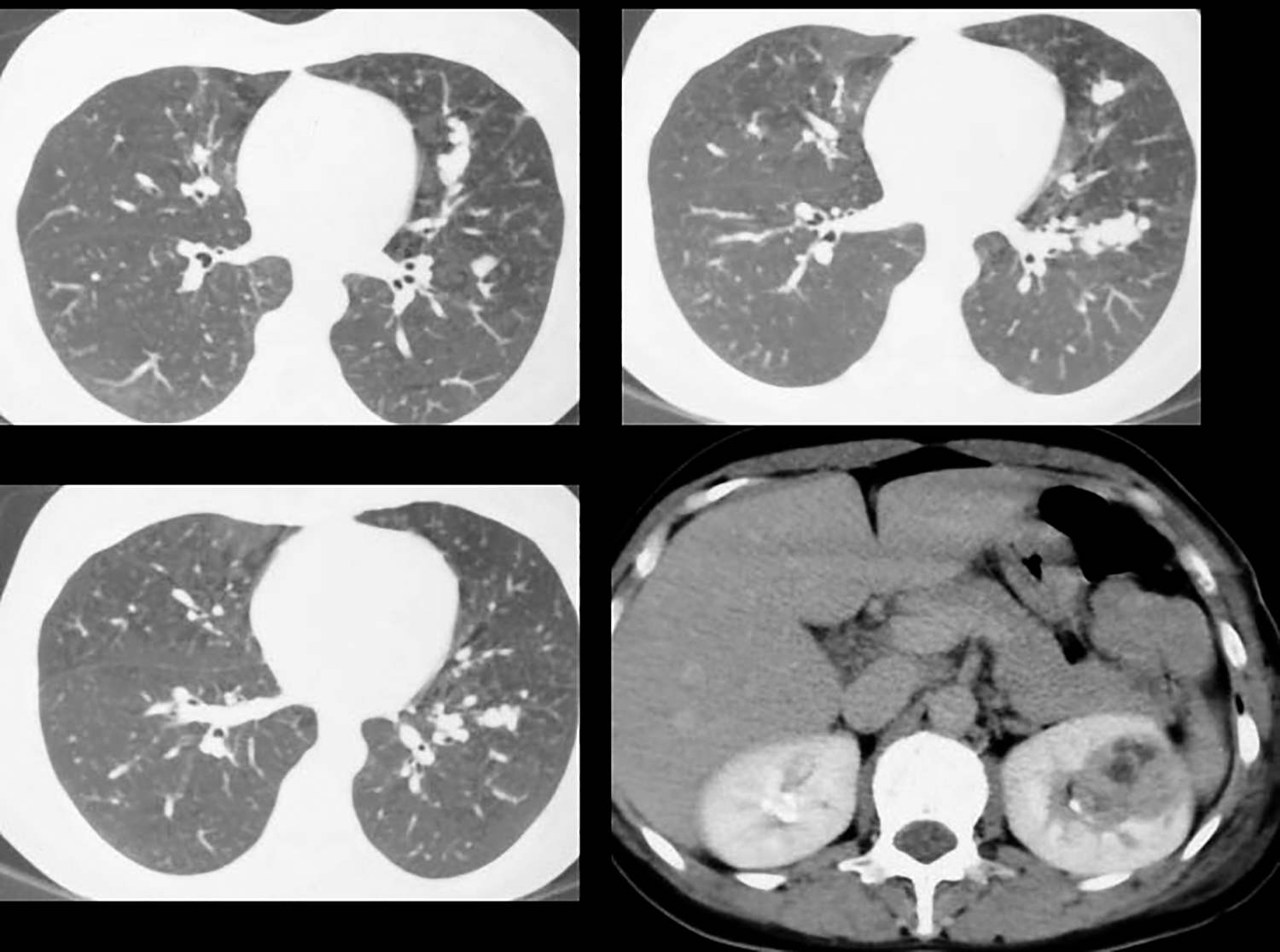
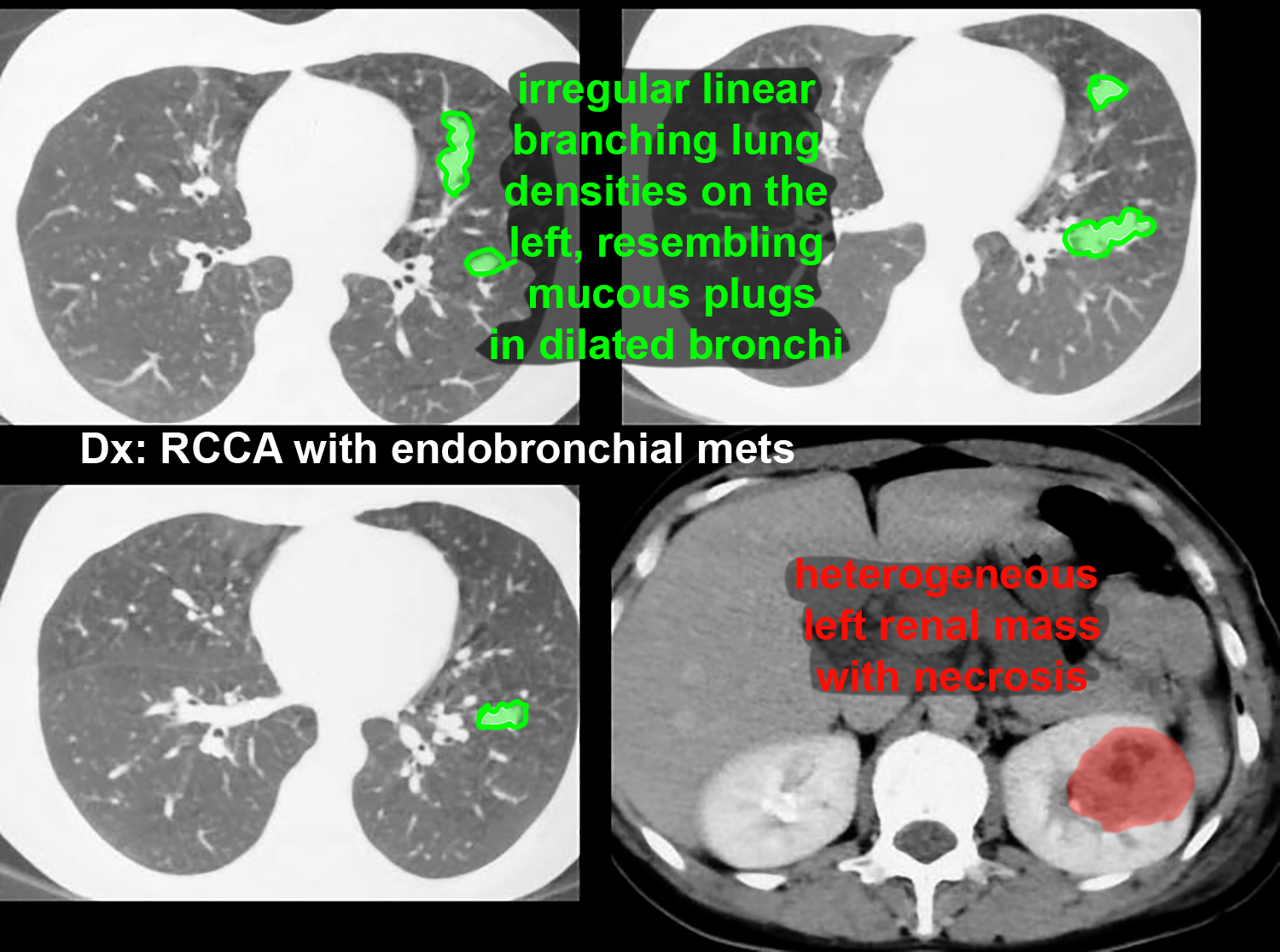
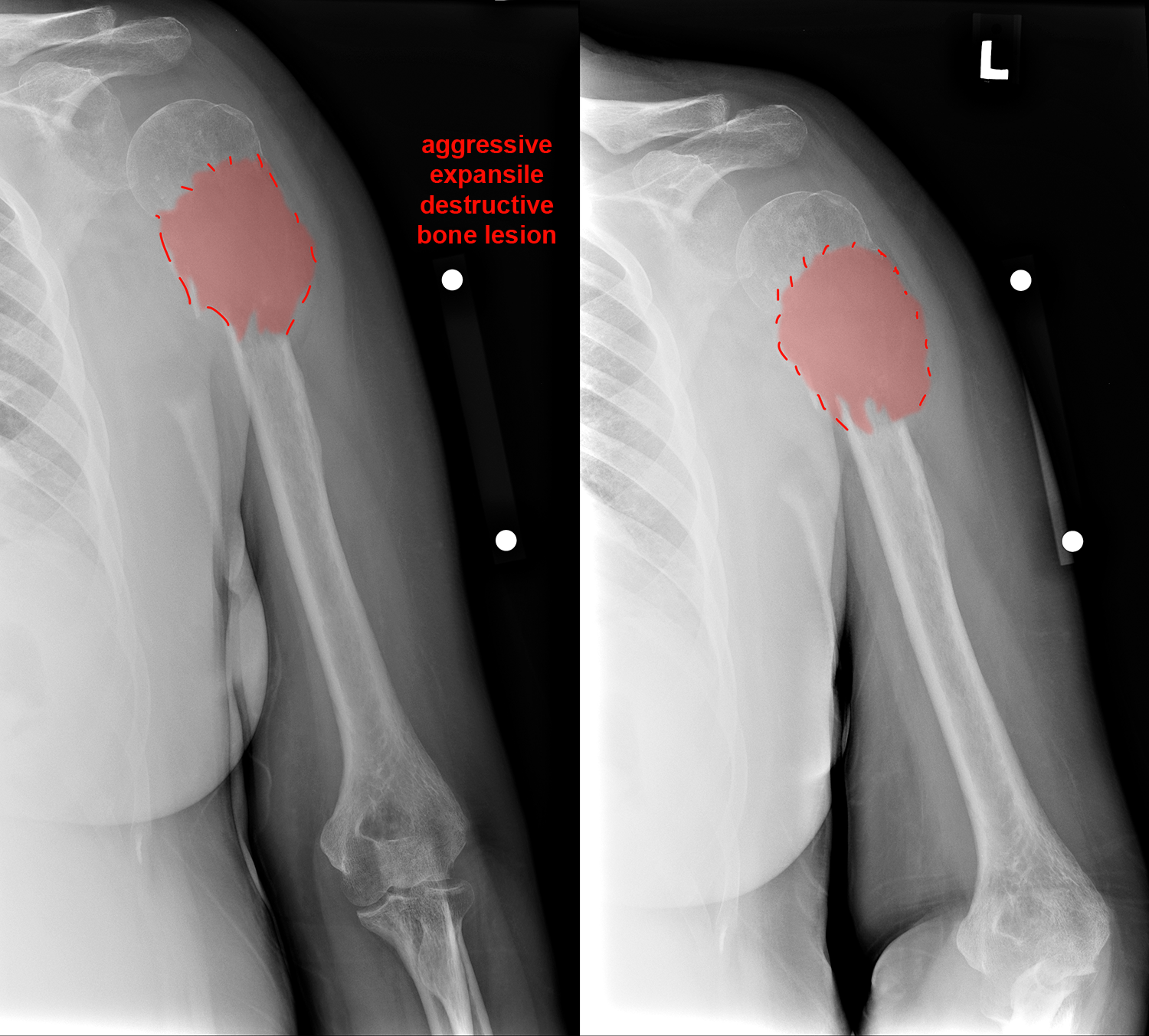
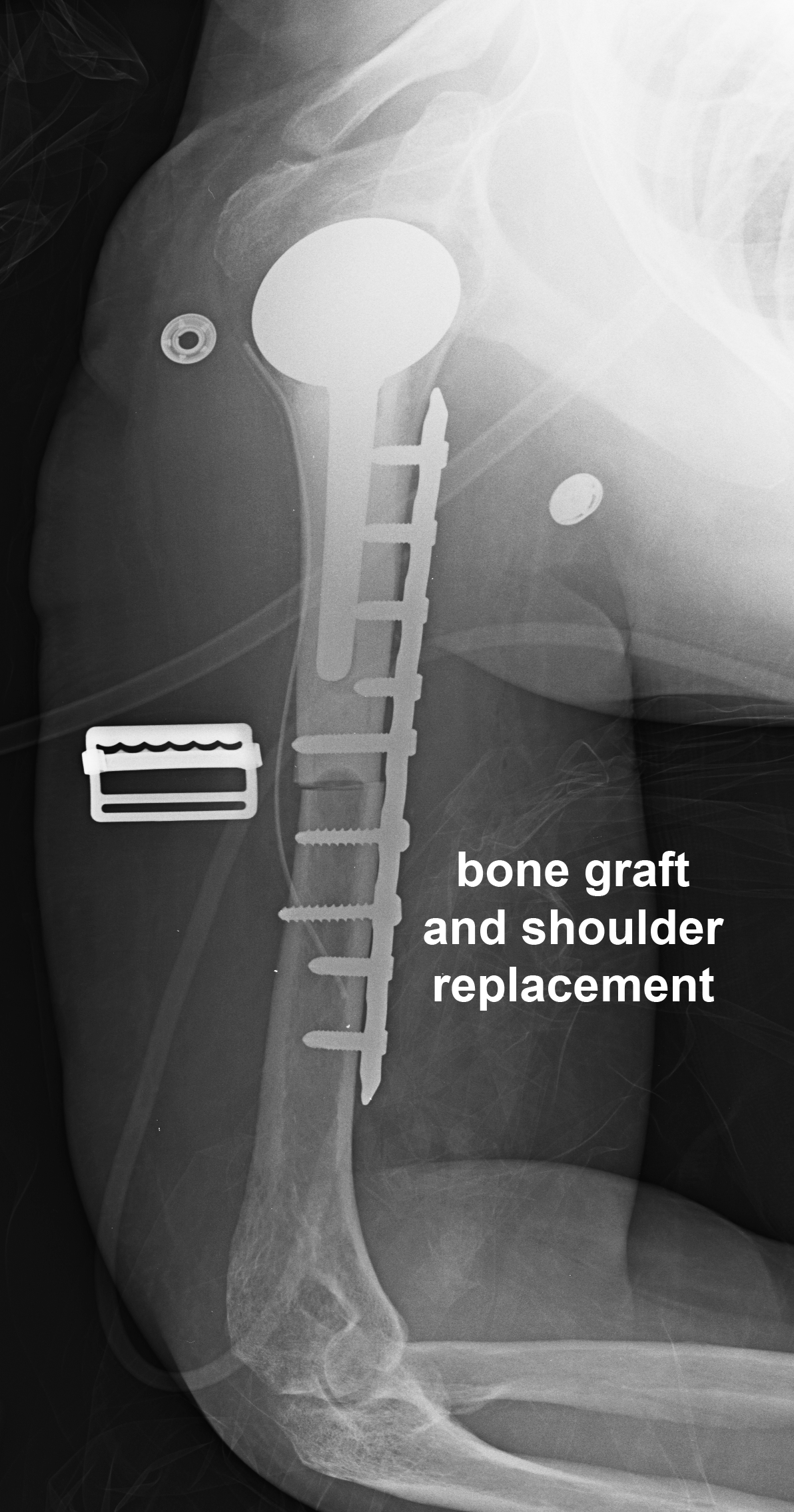
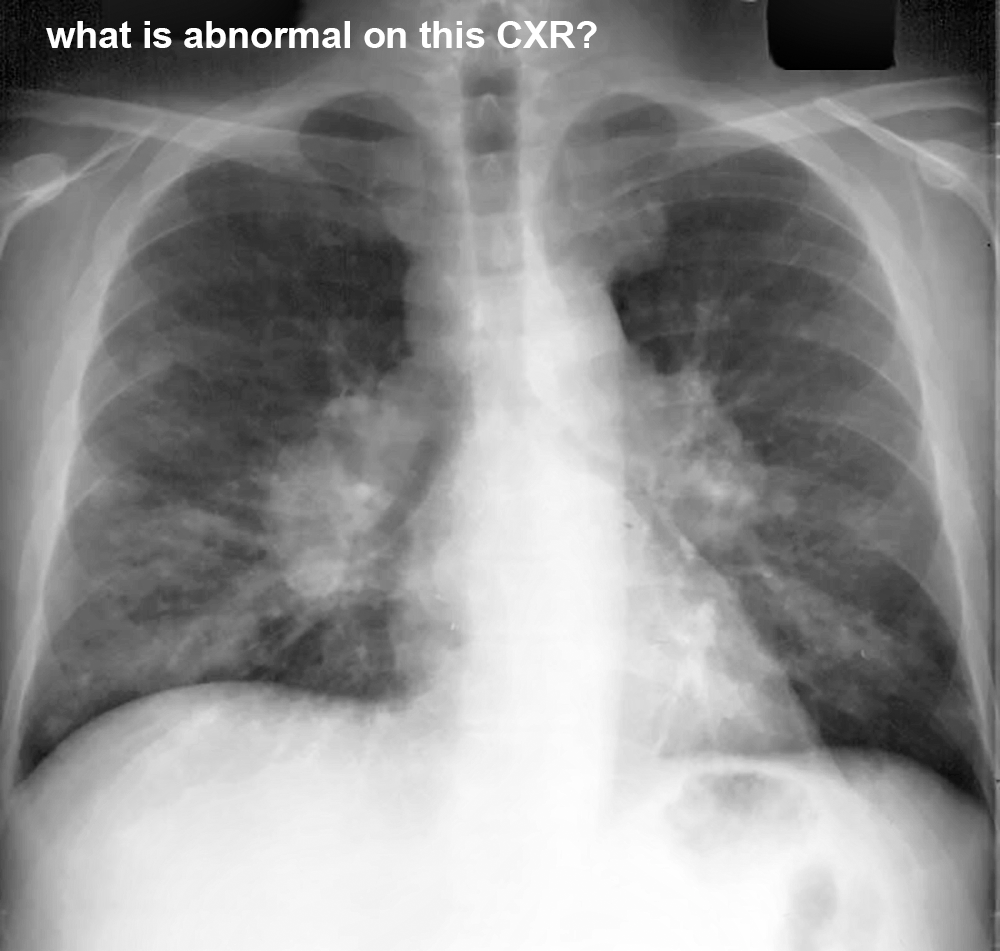
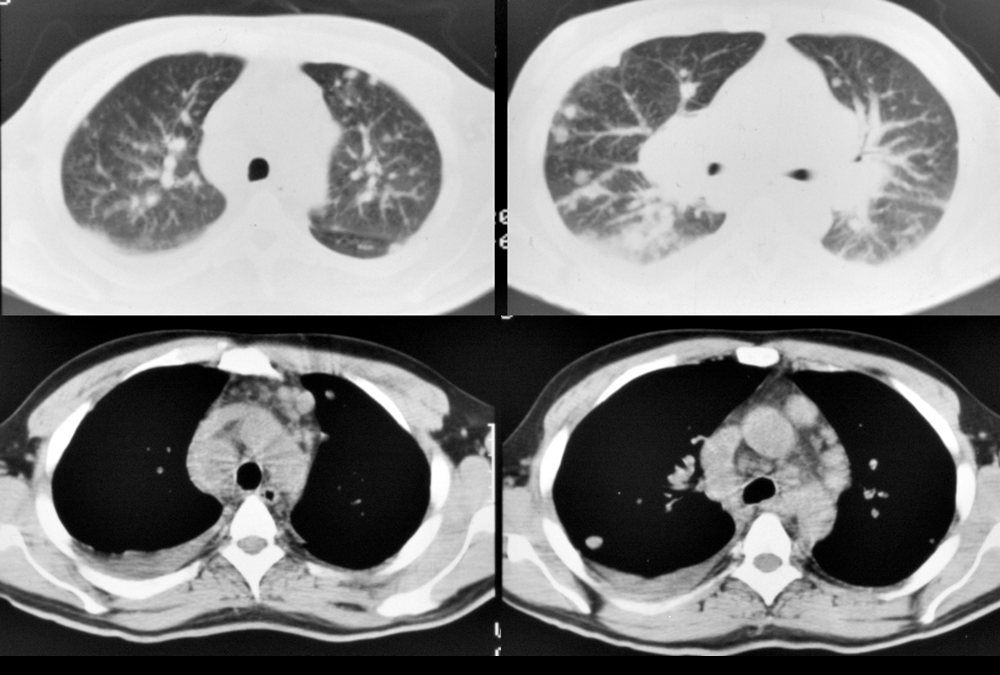
RCCA is a tumor with potential to metastasize to almost anywhere. It appears in most lists of unusual metastatic sites, such as thyroid, pancreas, skin, breast, endobronchial, skeletal muscle, and cardiac. Metastases can grow quickly and may be particularly destructive in bone. About 1/3 of patients quickly develop distant metastases after diagnosis and another 1/3 of patients have distant metastases at the time of diagnosis. With newer treatment options, metastatic disease can be managed more effectively. This page shows a common and an uncommon site for RCCA spread. The first patient presented with a cough.
Further Explanation: