













Case 1
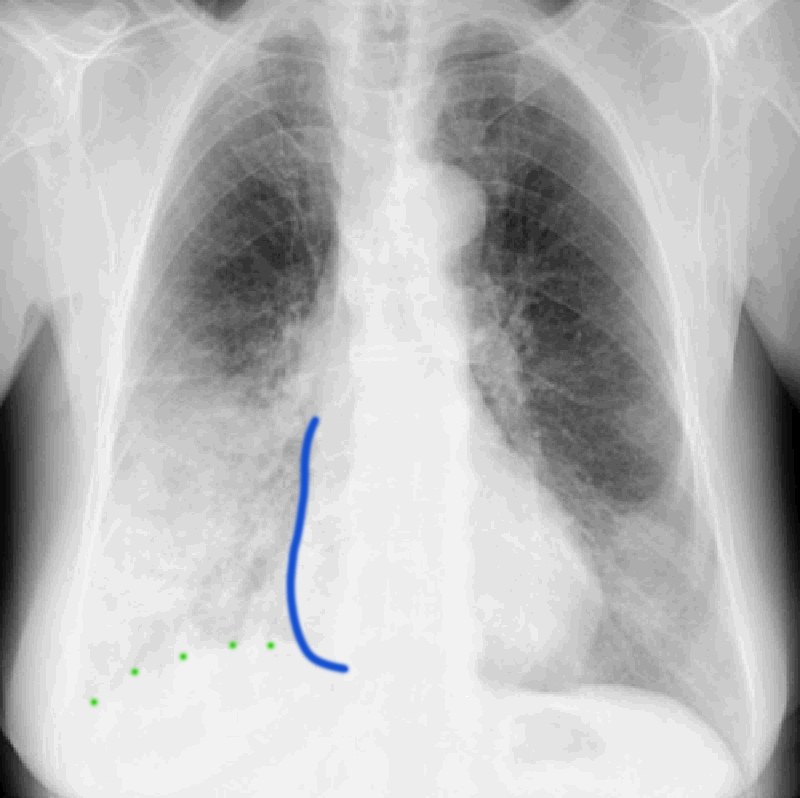
Case 1 provides a brief review of the anatomy of lung LOBES and FISSURES, and the appearance of processes that produce an ALVEOLAR pattern due to filling of airspaces. This radiograph is from a 65 year old woman with cough, fever, shaking chills and right pleuritic chest pain.
Question 1:
What lobe or lobes do you think are involved and what adjectives would you use to describe the abnormalities that you see? How does the appearance of the heart and diaphragm borders help you to localize the lung abnormalities?
There is hazy, ill-defined opacity that seems worst in the lower part of the right lung. This could involve either the lower lobe or the middle lobe or both. There is also less extensive opacity in the lower left lung laterally, either in the lingua of the left upper lobe or in the left lower lobe (or both). The right hemidiaphram (green dotted line) is almost completely obscured by the opacity, suggesting that the area of abnormal lung is abutting the diaphragm (mostly LOWER lobe). The right heart border (blue line) remains fairly well defined, suggesting that the lobe that abuts the heart (mostly MIDDLE lobe) is clear or less involved.


Case 1
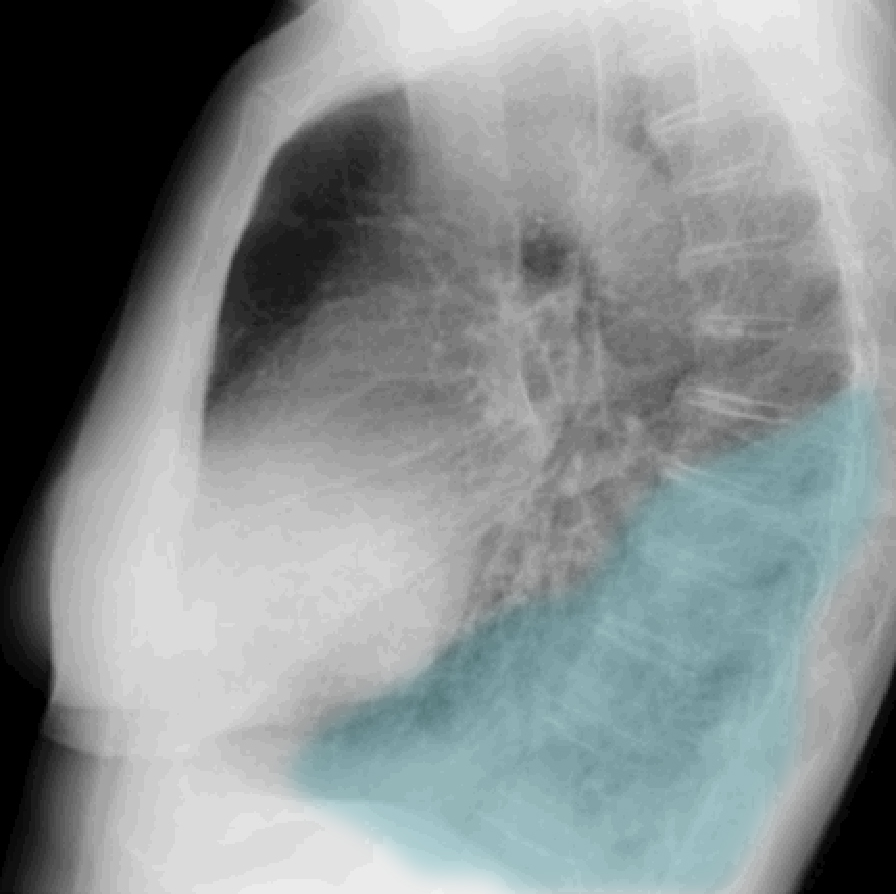
This is the next image on this patient.
Question 2:
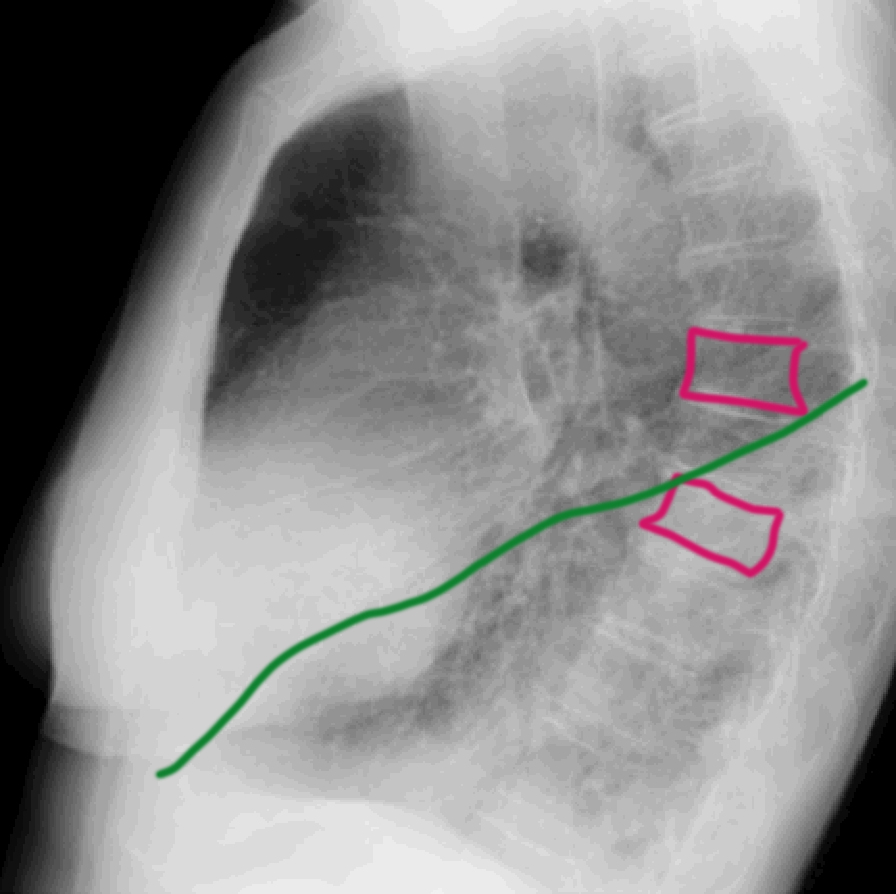
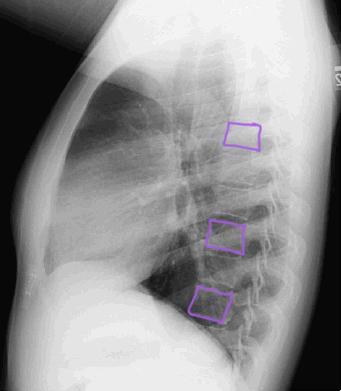
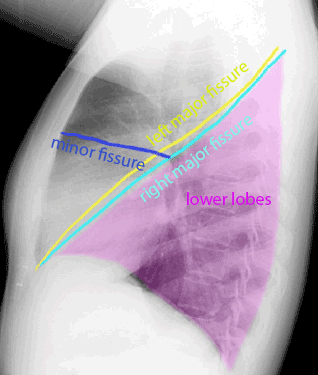
What is this view? Where is the lung abnormality located on this view? What do you think of the density of the vertebra in the upper vs lower thoracic region?
This is a lateral chest radiograph, typically done with the patient's LEFT side closest to the imaging receptor (called a 'left lateral' view). The abnormal opacity is relatively posterior in position on this view, consistent with LOWER lobe airspace disease. The finding can be more subtle on the lateral view than on the frontal view. This image shows the 'spine sign'. This is an indication of lower lobe lung disease as seen on the lateral view. If you view each level of the thoracic spine, each vertebra should look DARKER as you move inferiorly. In this case, as shown by the label (spine and fissure), you can see that as you move inferiorly, the spine becomes denser just below the level of the major fissure. This confirm presence of airspace consolidation (opacity) in the right lower lobe. Right middle lobe consolidation would be in a more anterior position on the lateral view, overlying the heart.

Case 1
This is the CT of our patient with symptoms of pneumonia.
Question 3:
What is the CT window used to display these images? What lobes are abnormal, and what anatomic part of the lung is involved?
These images are displayed with lung windows, meaning that the brightness and contrast have been optimized to show lung findings best (but are not ideal for viewing soft tissues or bones). The most impressive findings are in the right lower lobe, but other lobes are also involved. There are hazy opacities in the lingula (the lowest part of the left upper lobe) and in the right middle lobe. Hazy ill-defined opacities on CXR and CT suggest that the abnormality involves the airspaces of the lung. For the abnormal CT image with lobes labeled, red is the right upper lobe, yellow is the left upper lobe, green is the right lower lobe and purple is the left lower lobe. The slice is too high to include the right middle lobe. For the NORMAL CT with labels, the right upper lobe is green, the left upper lobe is purple, right right middle lobe is yellow, the right lower lobe is red and the left lower lobe is blue.



