Case 2
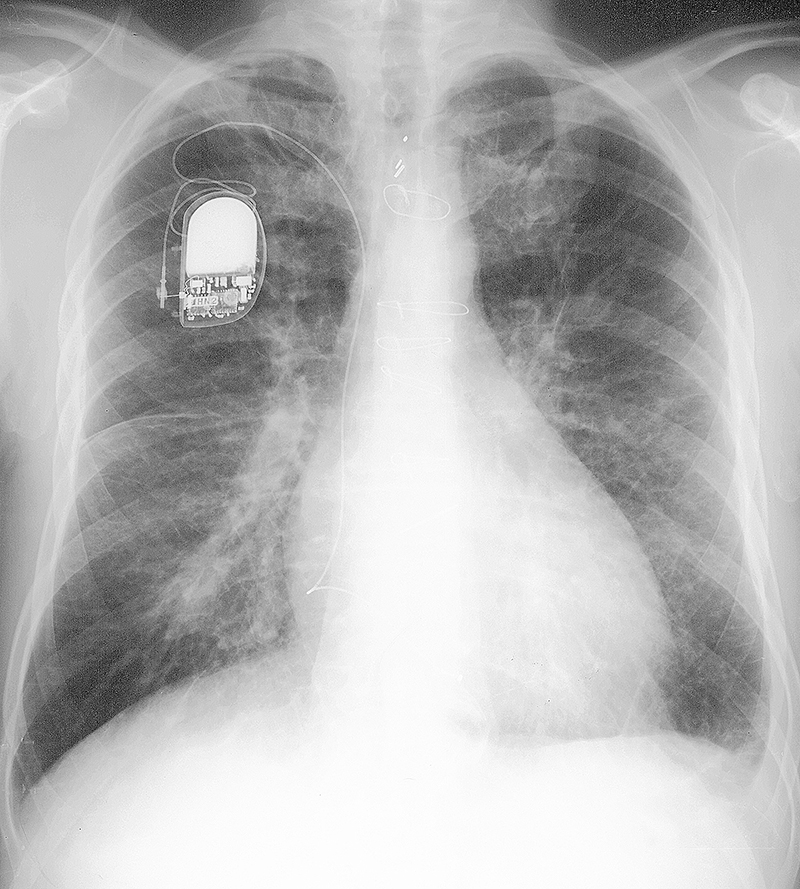
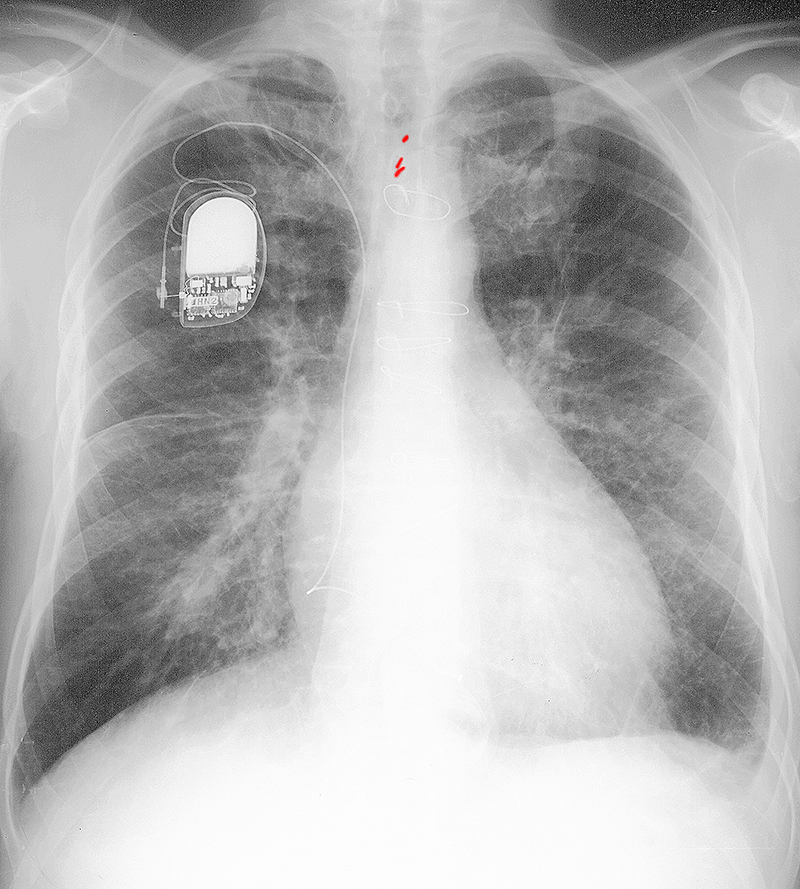
Case 2 reviews the patterns on imaging of abnormalities in the INTERSTITIUM of the lung. This radiograph is from a 71 year old man with chronic shortness of breath and a history of coronary artery disease and valve surgery.
Question 1:
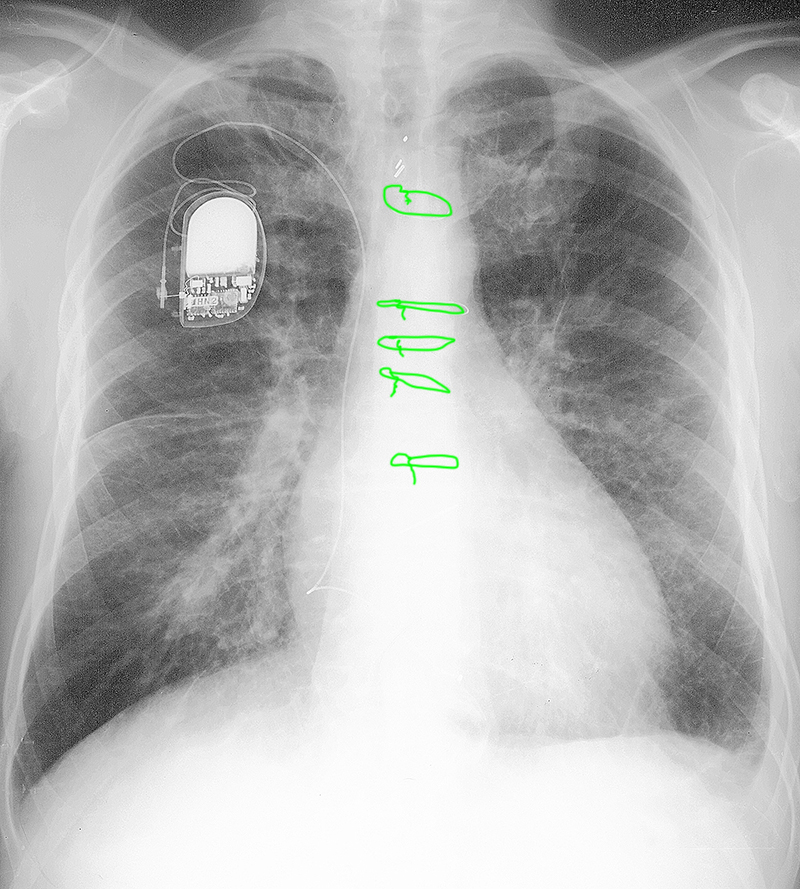
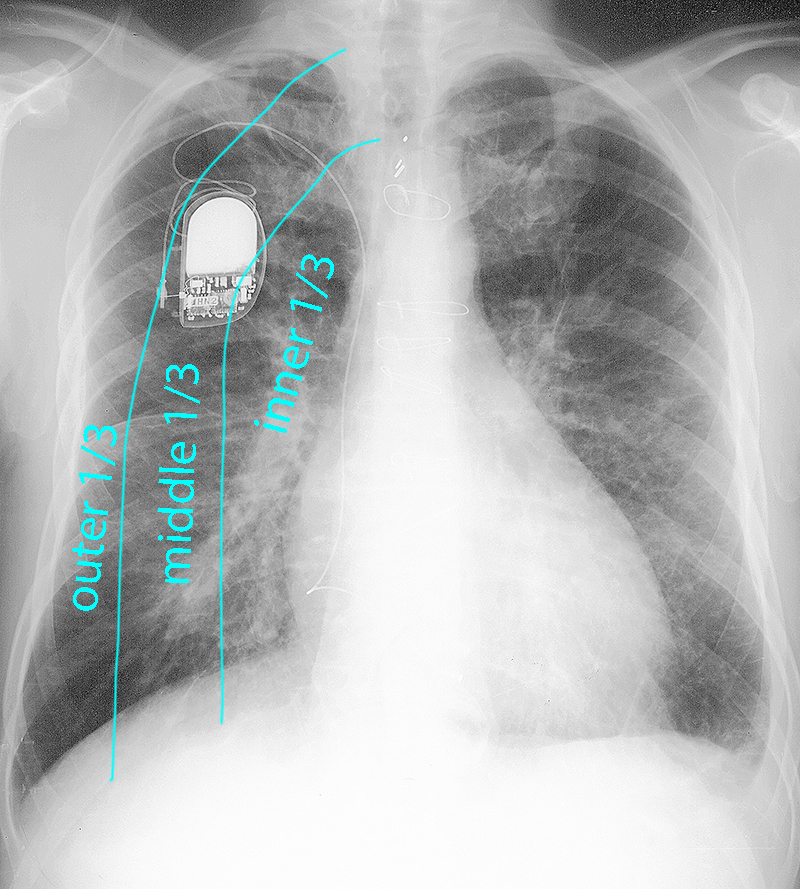
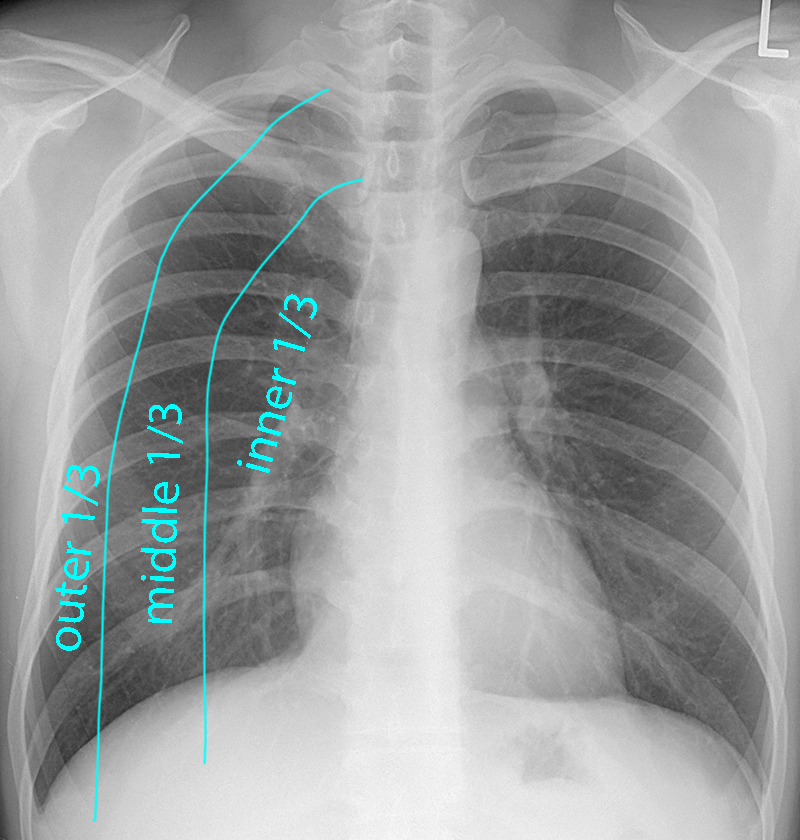
What adjectives would you use to describe the abnormalities in this patient's lungs? What should normally be seen in the three zones of the lung (indicated below)?
The lungs look like there are too many linear markings, particularly in the outer third where normal lung should be fairly dark, with only a few branching and tapering vessels visible. The pattern is of overlapping, criss-crossing lines, which can be called 'linear' or 'reticular'. Overall the markings are well-defined and not hazy, as in the previous case. In the inner zone of the lung, the pulmonary artery should be clearly seen with sharp margins (in our patient, the margins are not as sharp as normal, due to all the overlapping linear densities present). In the middle zone, you should be able to easily trace out next generation vascular branches (not so easy to do in our patient). In the outer zone, there should be very few visible markings (which is not the case in our patient, particularly in the costophrenic regions bilaterally where there are many parallel horizontal lines). The horizontal lines in the outer lung zone, particularly inferiorly, are called Kerley B lines.
Case 2
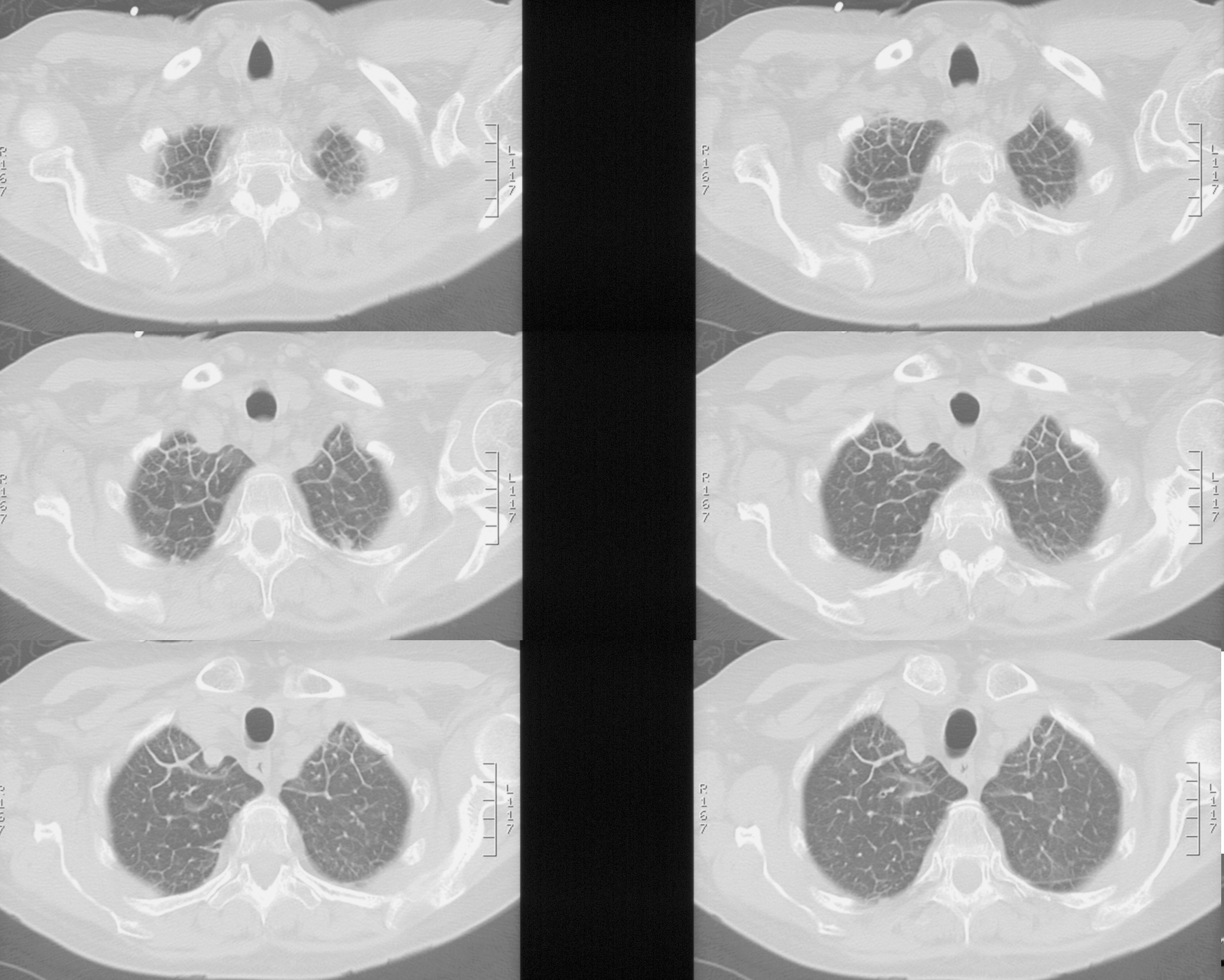
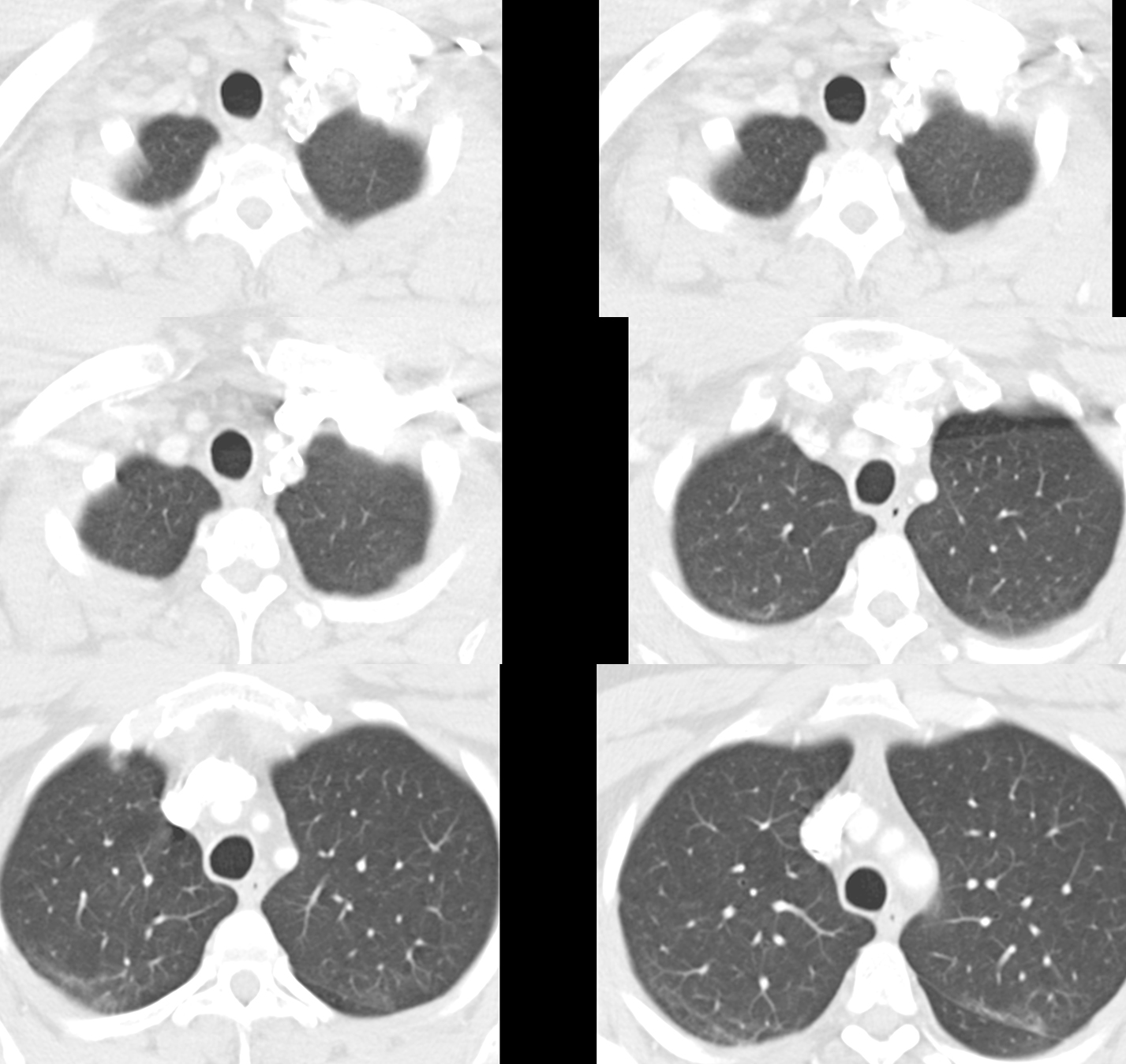
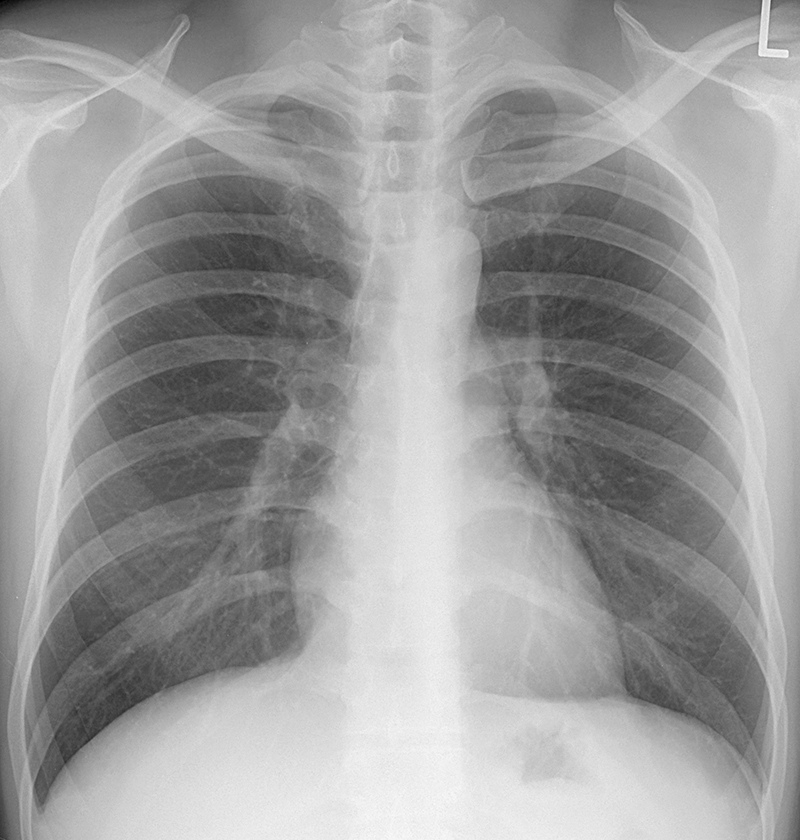
This is a set of CT images from a different patient, also with shortness of breath. You are shown a normal CT below for comparison.
Question 2:
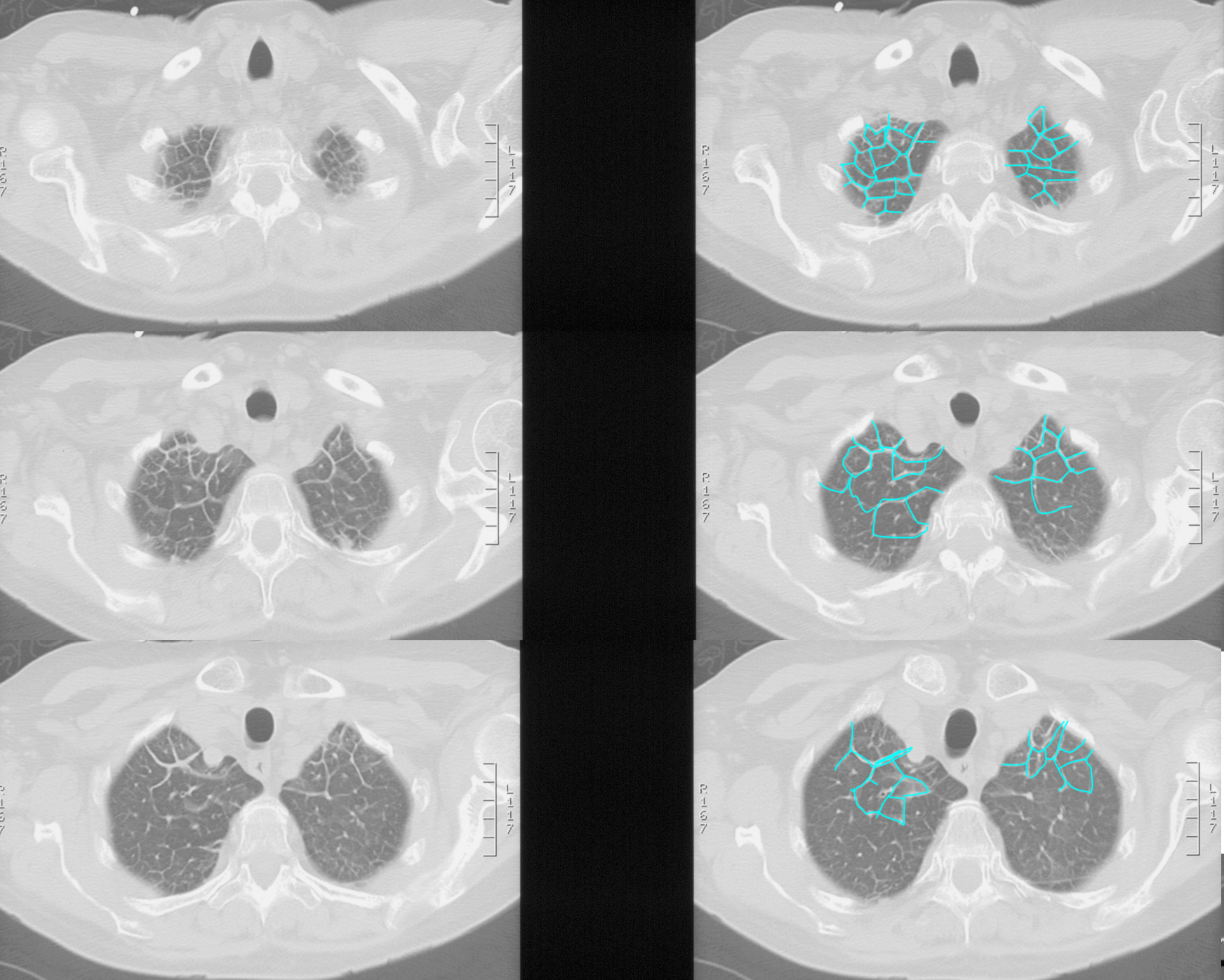
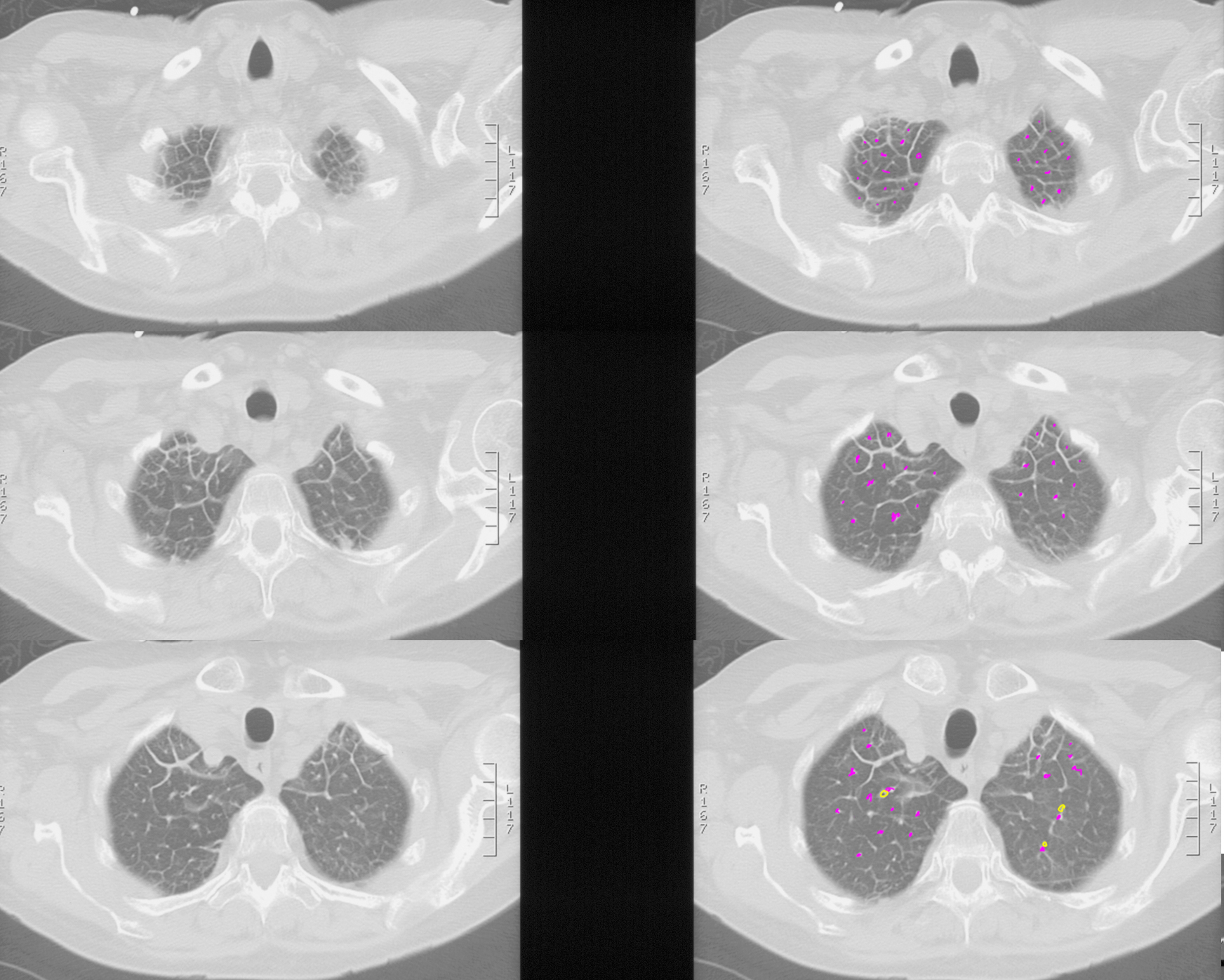
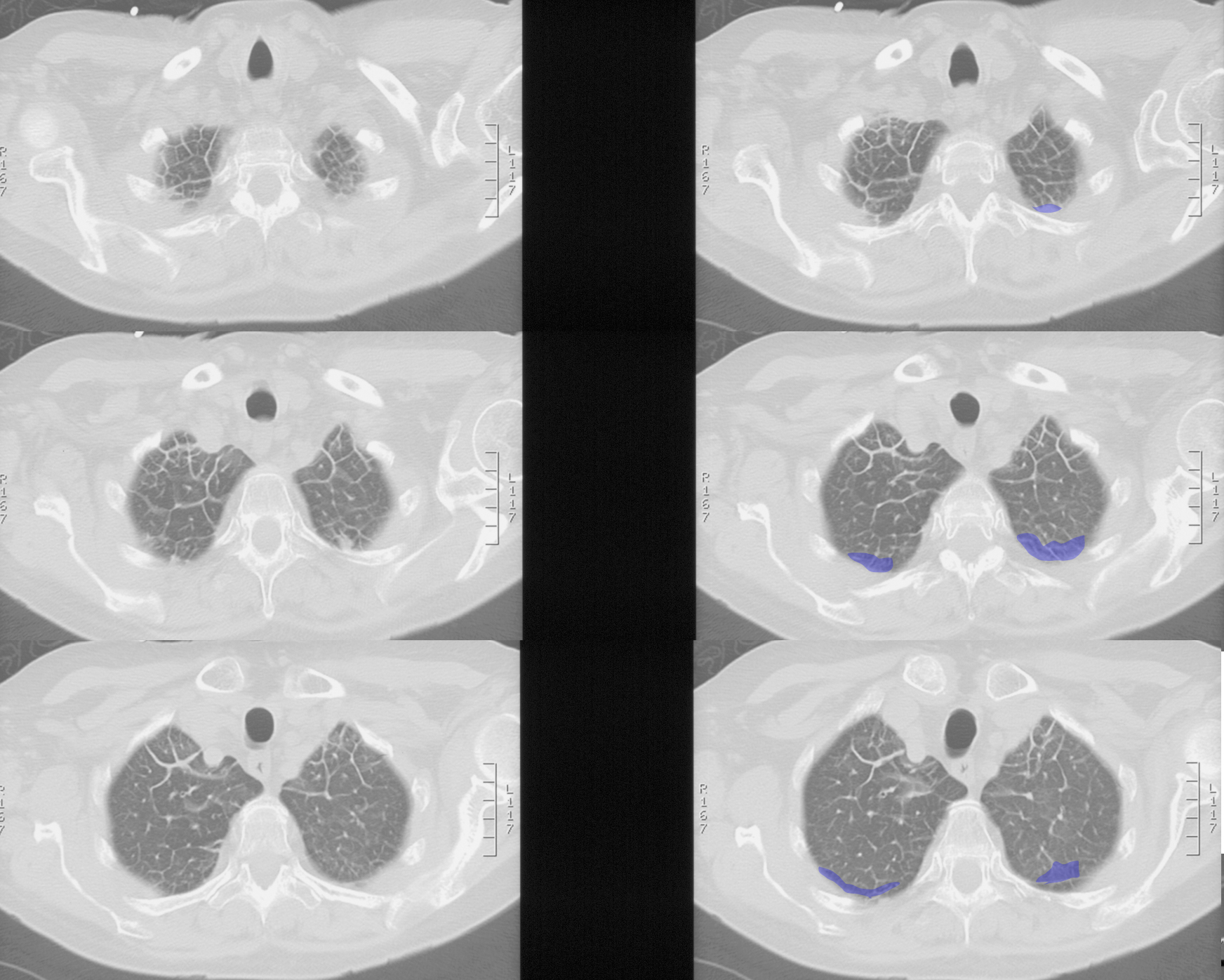
How would you describe the findings on this patient's CT images, and what does this appearance imply regarding what part of the lung is abnormal?
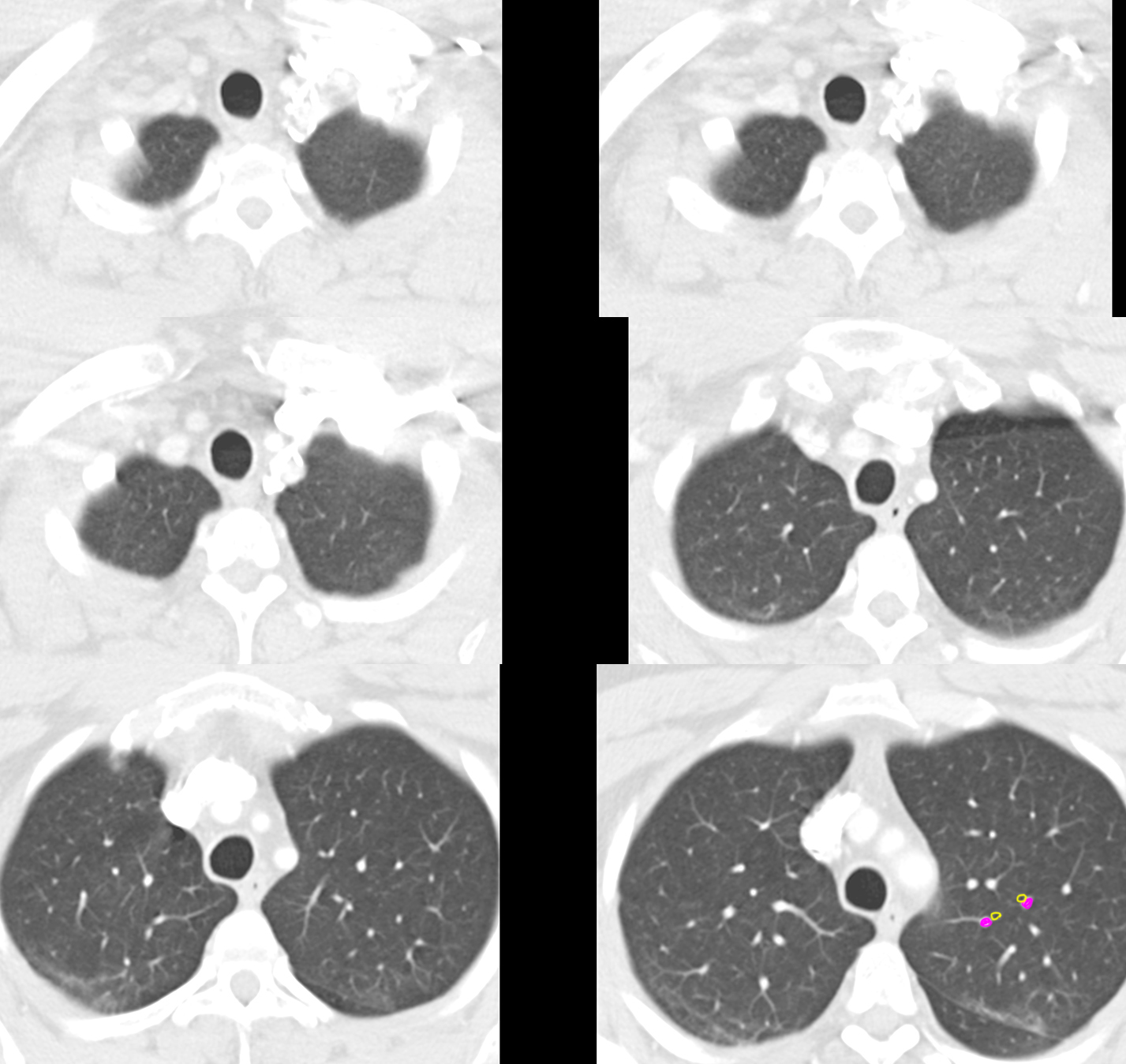
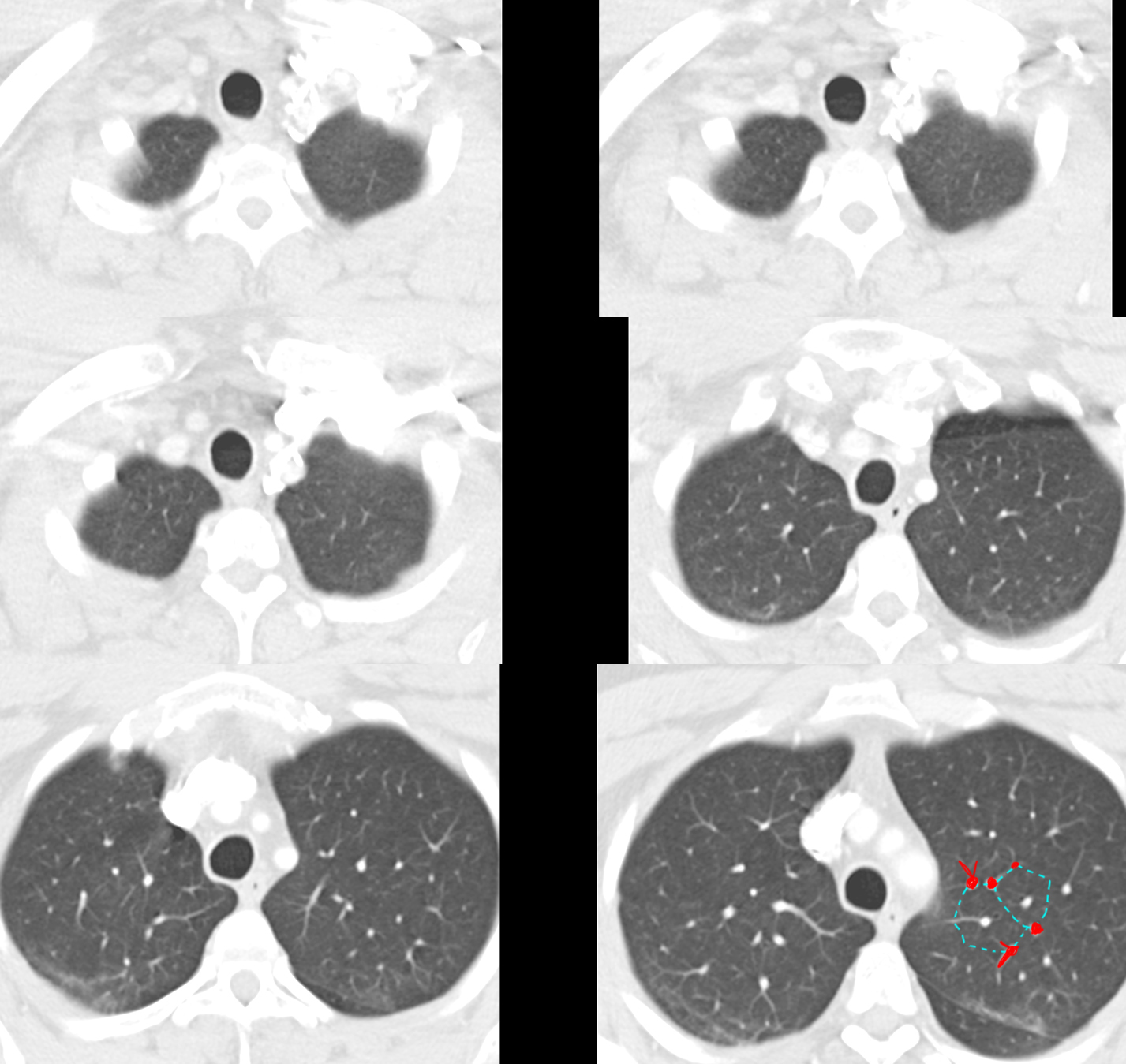
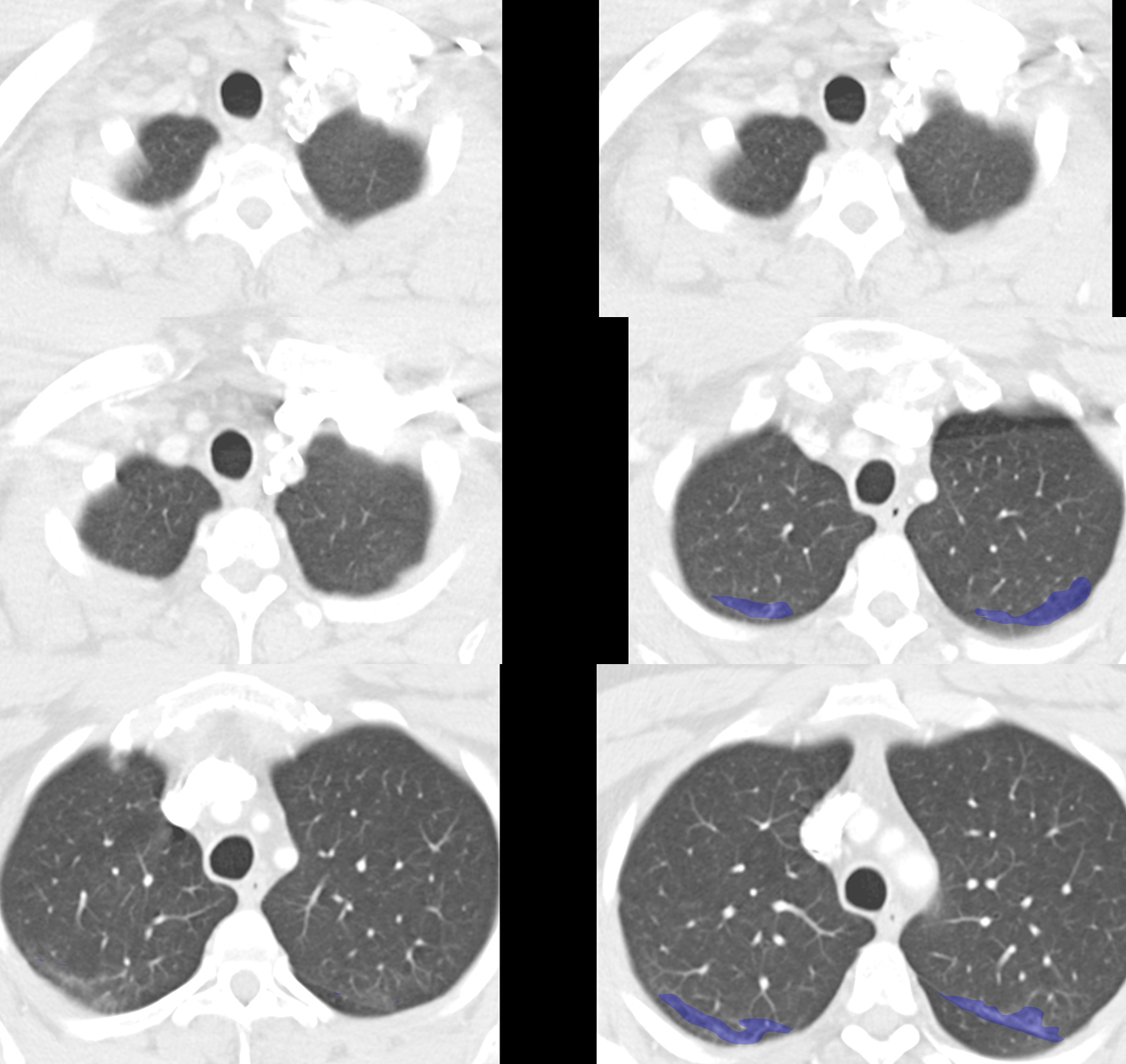
Again, in this patient as was seen on the CXR from the previous case, there are abnormal linear markings. On the CT, you can see that the markings outline polygonal regions of lung, about 1-2 cm in diameter. These markings represent thickening of the lung INTERSTITIUM. In this patient, these abnormally thickened interstitial elements seem to be mostly toward the upper lungs. In the prior patient, on CXR the most linear markings were in the bases.