Case 1
63 year old man with vague upper abdominal pain
Question 1:
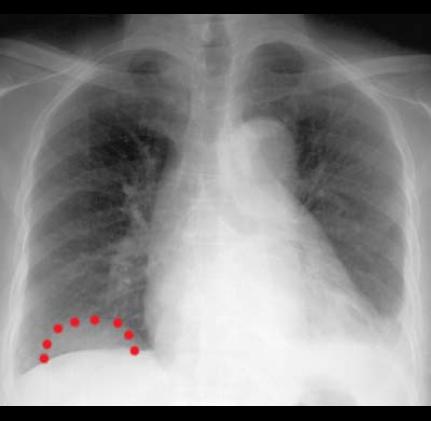
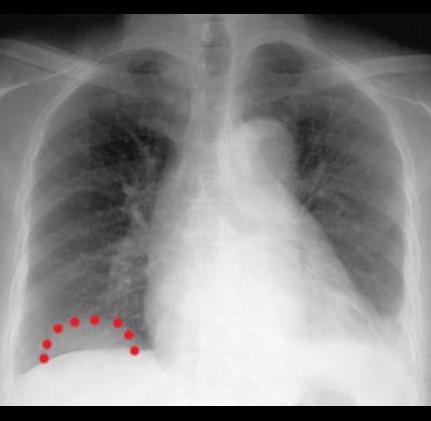
a) Two abnormalities are indicated by clicking on the links below. How would you describe the abnormality on the patient's right in terms of shape, density and margins?
The abnormality on the patient's right is round in shape with a relatively smooth, well-defined upper margin, although the lower part of the lesion is not well seen. Its density seems to be more than lung but less than abdominal contents or heart.
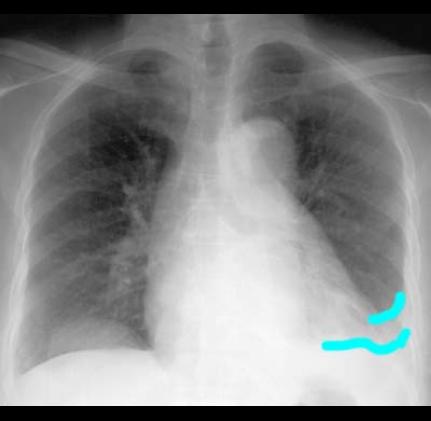
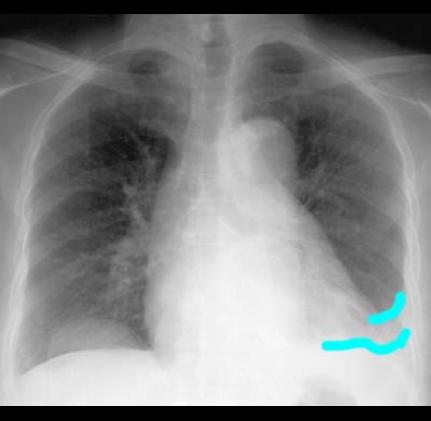
b) How would you describe the abnormality on the patient's left in terms of shape, density and margins?
The abnormality on the patient's left is not very well defined, with a suggestion of a concave shape (like a meniscus creeping up the inside of the ribs). It's density is more similar to heart or abdominal contents and it appears to be obscuring the normal contour of the left hemidiaphragm.
When describing findings on radiography, it is important to think about location, any structures that are displaced or obscured in the region of the finding, shape, margins (sharp, obscured, speculated), and density. On a radiograph, it is important to remember that density (as reflected by the shade of grey) is composed of a sum of all the tissues that the beam went through to reach that group of pixels. This is different from a sectional radiographic study like CT, where the thickness of the image is relatively thin, so the actual shade of grey is a closer representation of the actual tissue present in that part of the image. So when considering density of a finding on radiography, it is more useful to compare it to adjacent structures for a 'relative' density estimation.

Case 1
This is the same image previously shown on our patient. The finding on the right can be called a mass. The shape and configuration of the left finding is most consistent with a pleural process.
Question 2:
a) Where are a few locations of origin for the mass on the patient's right?
Given that its location straddles the diaphragm, you could consider sites above, within, or below that structure. So this could be arising from the lung, the pleura (above), the diaphragm itself, or the peritoneum, liver or kidney (below).
b) What could be causing the findings on the patient's left?
Since the shape suggests location in the pleural space, you could consider a transudative effusion (watery), an exudate (like infection or empyema), hemorrhage, tumor, or fibrosis.
It is often a good idea to start your analysis of imaging findings BROADLY, beginning with the features previously noted (shape, margins, density, location, effect on adjacent structures), and then use the patient history to narrow things down.

Case 1
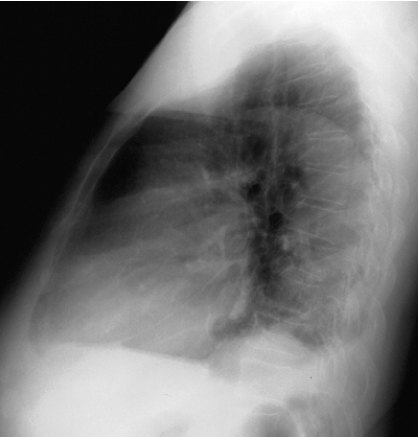
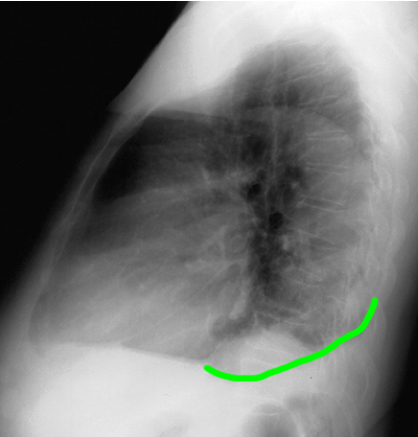
This is another image of the same patient. Try to identify the abnormalities that were seen on the prior frontal view.
Question 3:
a) What is this view called?
This is a lateral radiograph of the chest. It can be displayed facing to the left or to the right. There is no established standard for this, so it varies from one place to another.
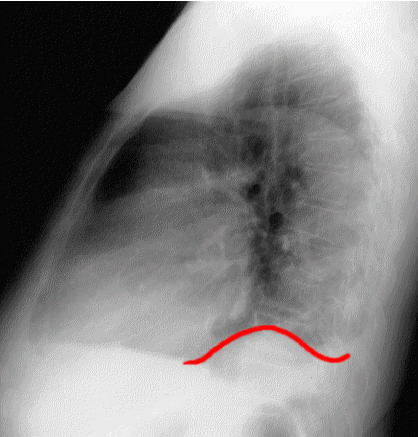
b) Where is the lowest part of the pleural space in the upright position?
The pleural space extends far down in the back (posteriorly), so the posterior costophrenic (costodiaphragmatic) recess is the lowest. So we expect to see small pleural effusions best on the lateral view.
c) What is the next study you would consider ordering?
When there are confusing abnormalities on a chest radiograph, CT is usually the next study to order.
What do you call an abnormality where a structure is protruding through an abnormal opening into an unusual location?
Case 1
This is the next study that was done in this patient.
Question 4:
a) What is this study? Be specific.
This is CT scan of the lower chest and abdomen. It is displayed in the axial plane with soft tissue windows (fat and muscle look very different in terms of shades of grey), and there is no IV contrast present (large vessels like the aorta are the same shade of grey as muscle).
b) Can you locate the mass on the patient's right side? What do you think it consists of?
If you scroll through the CT images, you will see the mass appear on the lowest cuts. It seems to consist of fatty density surrounding a well-defined soft tissue structure with faint fat in its center. This orderly arrangement would be very unusual for a tumor. This represents the kidney, herniating across the diaphragm.
Case 1
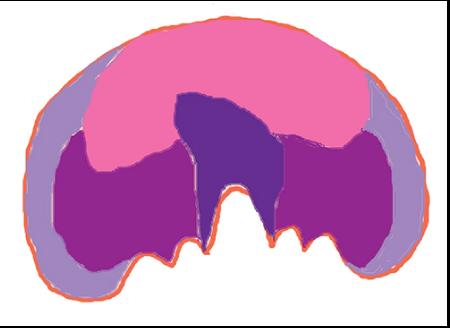
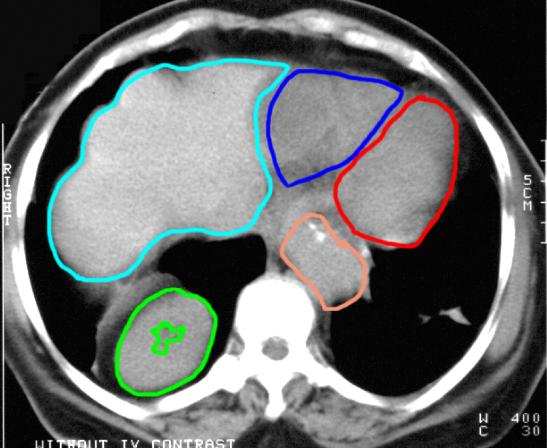
This is the lowest cut from the previous CT scan. Try to identify the outlined structures. The answers are on the next image.
Question 5:
a) How does the radiation dose for a CT scan compare to that of a KUB?
There is about an order of magnitude more radiation from a CT scan than a radiograph.
b) Does the scan protocol for a CT affect radiation dose?
Yes, in particular if a part of the body will be scanned multiple times (for example, if the CT is ordered both without and with IV contrast), that will increase the dose. The highest dose is when a scan is performed at multiple points after before and after contrast, which is sometimes done to evaluate vascular anomalies or tumors.
Case 1
This is a study from a different patient with a similar problem.
Question 6:
a) What are technical parameters for this study?
These are coronal CT images, displayed in soft tissue window, with IV contrast. Note how bright the heart chambers and large vessels are compared to muscle.
b) How much extra scan time is needed to obtain this image plane and how much extra radiation is the patient exposed to?
NONE! The patient is scanned in the axial plane, but the coronal images are reconstructed by the computer after the scan is done. No extra time for the patient is needed and there is no extra radiation dose for these additional images in different planes.
The labeled structures on the prior CT image were the liver (aqua), the right ventricle of the heart (dark blue), the left ventricle of the heart (red), the stomach (orange) and the right kidney (green).
When a structure is protruding into a space where it is not normally located, this is called a 'hernia'. There can be hernias in many parts of the body. Since the diaphragm is a relatively thin structure, hernias through the diaphragm are not uncommon through weak points, or related to trauma. The type of hernia that these two patients have (with abdominal contents crossing upward in the posterior-lateral part of the diaphragm) are called Bochdalek hernias, named for a Bohemian anatomist. This type of hernia can happen in neonates, and can sometimes be large enough to affect their breathing. When they are found in adults, they are often smaller and relatively asymptomatic. This particular patient has quite a large Bochdalek hernia on the left, which may well compromise his left lung function somewhat. However, he was relatively asymptomatic. The first patient had a smaller Bochdalek hernia on the right and his symptoms were not likely related to that, but more likely were due to his left pleural disease.
Case 1
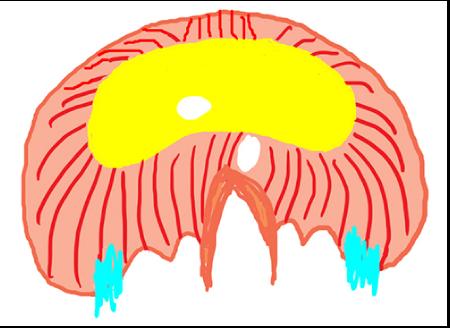
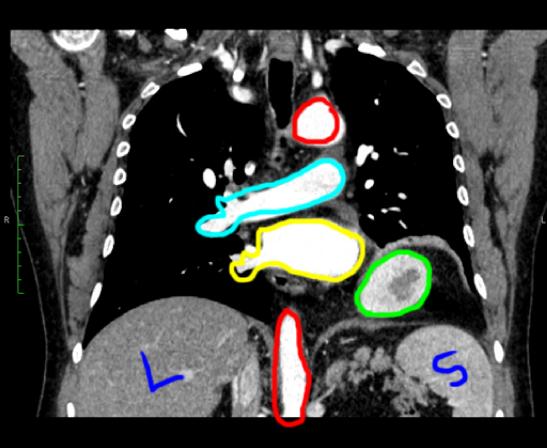
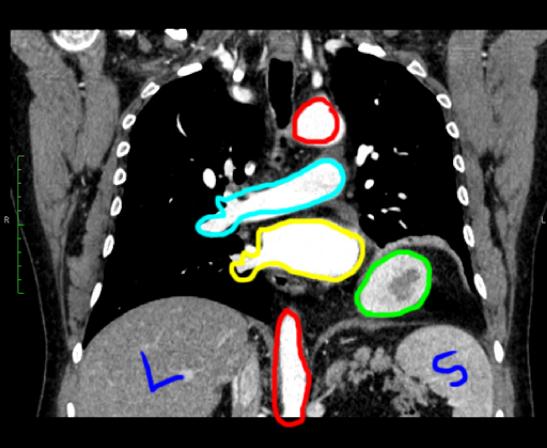
This is a select coronal CT image from the second patient. Try to identify the labeled structures.
Question 7:
a) How are the patient's arms positioned for a chest CT?
They are usually overhead, as you can seem from this image looking at the position of the lateral chest wall muscles. This is to make the body more tubular overall in shape, which decreases artifact from having the beam go through a very flattened oval (as the chest and shoulders typically are if the arms are at the sides).
b) How are the patient's arms positioned for an abdomen CT?
They are usually also overhead, but as the abdomen is already fairly tubular in shape, sometimes they are at the sides or across the chest. And of course, they would not be elevated in the setting of trauma or injury to chest wall or shoulder or upper extremity.
Case 1
This is the same labeled coronal CT image. Red is the aorta (upper part is the arch and lower part is the junction of thoracic and abdominal descending aorta), aqua is right pulmonary artery, yellow is left atrium (with some right lung pulmonary veins joining), green is the left kidney. Spleen (S) and liver L are also labeled.
Question 8:
What nerve supplies the diaphragm?
The phrenic nerve, arising high up in the neck from C2,4 and 5. It travels down along each side of the mediastinum, passing anterior to the pulmonary hilum to reach the diaphragm, which it pierces and spreads out on the deep surface.
Case 1
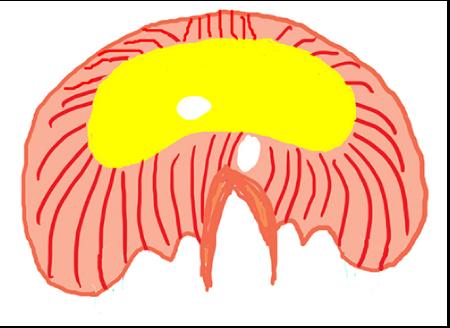
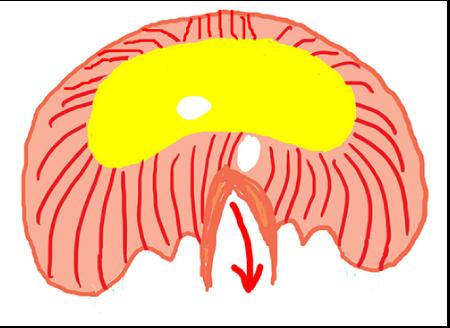
This is a diagram to review the complex embryology of the formation of the diaphragm, as well as the various structures that normally pass through the diaphragm.
Question 9:
a) Why is the diaphragm prone to development of hernias?
If the various embryologic components that make up the normal diaphragm do not quite fuse normally, it can leave weak spots. Also, since various holes are required to let structures pass through, these can also lead to development of hernias.
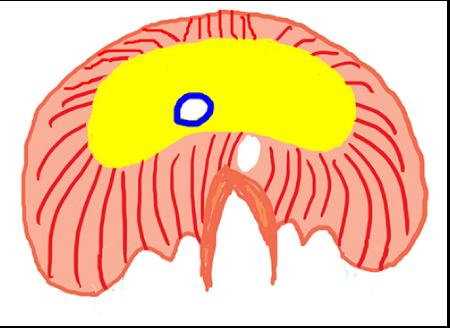
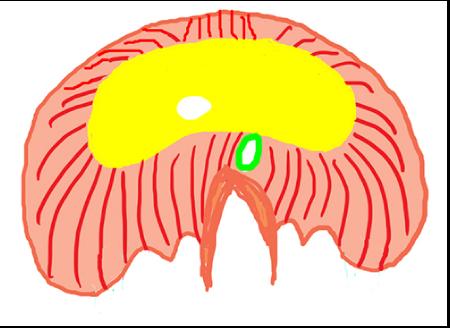
b) Which normal opening in the diaphragm is most prone to developing hernias?
The opening for the esophagus is often a site for hernias, called 'hiatal hernias'. In this situation, the stomach can herniate upward into the chest and this can lead to problems with normal closure of the lower esophageal sphincter. This can result in acid reflux into the esophagus and heartburn.