Case 2
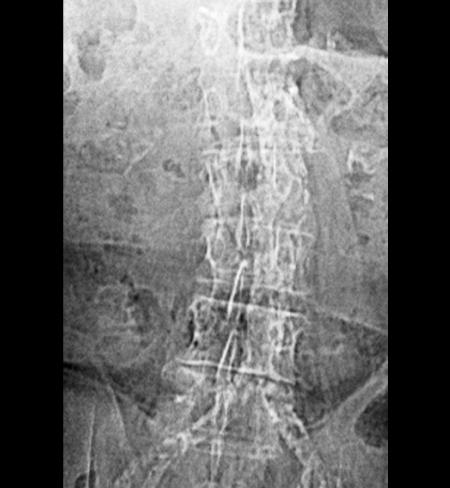
This is an image from a 78 year old man with pain in his legs after walking and occasional abdominal pain after large meals.
Question 1:
a) What type of study is this? Be specific.
This looks like a radiograph of the abdomen, but the image quality seems very poor. In fact, this is a low-quality type of radiograph performed at the beginning of a CT scan for localization only, called a 'scout' or 'scanogram' or 'topogram'. It does not have the same resolution and contrast that a regular abdominal radiograph would have, but it is still an x-ray image.
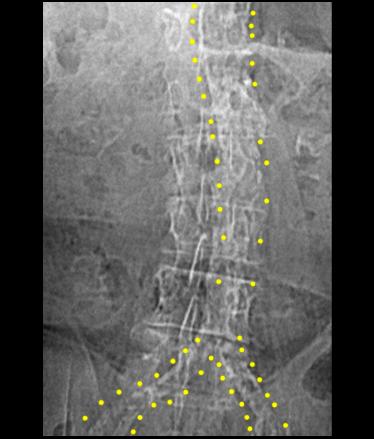
b) Looking at the labels below, what do you think is the mystery structure?
The yellow dotted lines seem to be outlining the abdominal aorta and its bifurcation. But the aorta is not normally visible on a radiograph, so this is abnormal.

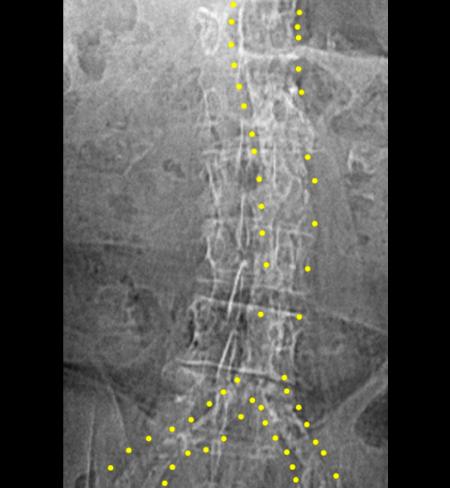
Case 2
This is the same image as previously shown. Think about what might make the vascular structures visible on this image, and how this might correlate with the patient's symptoms (leg pain after walking, abdominal pain after eating).
Question 2:
a) What is a term used for a radiograph of the abdomen?
A radiograph of the abdomen is often referred to as a KUB (for kidney, ureter and bladder), for short. Obviously there are more organs than this in the region being imaged.
b) Are the kidneys, ureters and bladder generally visible on an abdominal radiograph?
NO! So some people object to using the term KUB to refer to an abdominal radiograph, but it is short, easy to say, easy to write, and universally understood, so it is still a common abbreviation for this type of image.
c) How is the patient positioned for an abdominal radiograph?
They are in the supine position, unless some other specific position is requested. A KUB can be done upright, decubitus or prone, if requested, but if no specific positioning is requested, it will be done supine.
Case 2
The scout image shown previously was done prior to the study shown here.
Question 3:
a) What type of study is this (be specific)?
This is an axial CT scan of the chest and upper abdomen, displayed with soft tissue windows (muscle and fat are very different shades of grey and internal structure of bones is not well seen), without IV contrast (blood in the lumen of the heart and aorta is the same shade of grey as muscle).
b) Do you see an explanation for why the abdominal aorta was visible on the scout image?
There is dense calcification in the walls of most of the large arterial vessels of the mediastinum and abdomen. This is consistent with severe atherosclerosis.
c) How could this relate to the patient's symptoms?
Calcification in the walls of arteries can lead to narrowing and decreased blood supply. With exercise (such as walking), normal vessels can respond with increased flow, but atherosclerotic, narrowed vessels cannot, leading to pain. Similar pain can occur in the GI tract for the same reason after large meals.
Case 2
This is the same axial CT series shown previously.
Question 4:
a) Why was no IV contrast given?
There are many potential reasons that IV contrast might not be given, including renal failure or history of allergy to CT contrast material. In this case, the calcification in the vessel walls might be partly obscured if contrast was given, but that is usually not a contraindication to its use.
b) What other type of study can be done to define areas of narrowing (stenosis) of vessels?
Angiography can be done, particularly if there is a plan to intervene to try to open up narrowed areas. CT images can be processed to produce images that look very similar to angiograms, but if intervention is planned, then angiography is needed.
Case 2
This is a study on a different patient. The images are normal.
Question 5:
a) What is this study called?
This can be called an 'angiogram', which is the least specific term, but still correct. If you know what vessel is being shown, you can use a more specific term. If you know it is a study of an artery, you can call it an 'arteriogram', and if you know what vessel it is, you can use that name.
b) What vessel has been injected?
This is the celiac artery, so the most specific term would be a 'celiac arteriogram'.
c) What part of the body is supplied by this vessel?
The celiac artery is the main vessel to the foregut (other than the mouth and esophagus), from the gastro-esophageal junction to the point at which the common bile duct enters the duodenum.
Case 2
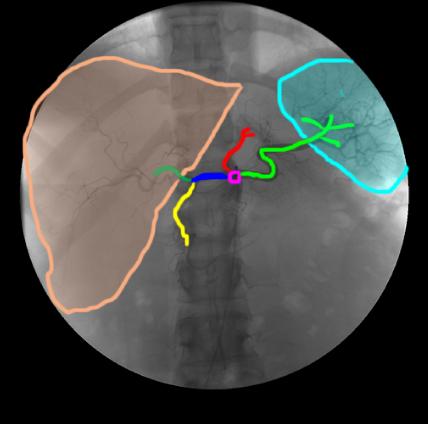
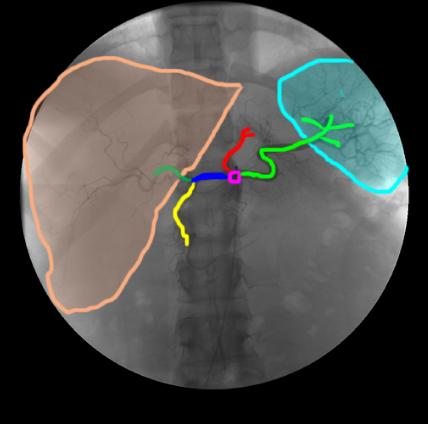
This is a selected image from near the end of the previous angiogram of the celiac artery. Various parts of the vessel and associated organs are outlined for you to identify.
Question 6:
a) What vessel was likely used to access the vascular system for this study?
If you check the catheter label below, you can see that it seems to be coming from below to the patient's right, so the likely vessel of access is the right femoral artery.
b) What complications can a patient experience after a procedure such as this?
They can develop bleeding and a hematoma at the femoral artery access point. They can also develop clot at the access point, which can compromise blood flow to the leg. Both are serious complications, but thankfully rare.

Case 2
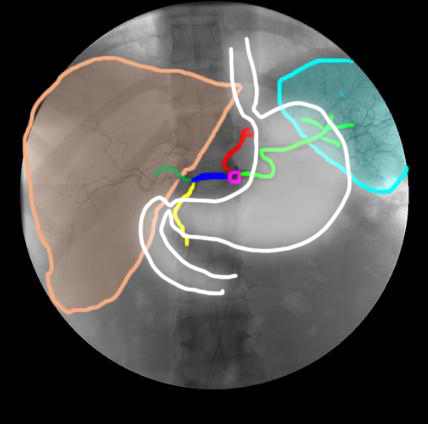
This is the same image from the celiac angiogram shown before. Click below to see the approximate location of the stomach, which will help with identification of structures.
Question 7:
What color is the contrast on these angiographic images?
It is dark (which is the opposite of the way we are used to seeing contrast on other types of x-ray studies, like CT scans and GI fluoroscopy. This is because many angiographers prefer to look at 'inverted' images. It is just a setting on the display. So by pushing a button, we can make the contrast appear white (see the link below) if we prefer.
The liver is shown in orange. The spleen is shown in aqua. The short end-on celiac trunk is shown in purple. The left gastric artery is red, the splenic artery is light green, the common hepatic artery is dark blue, the proper hepatic artery is dark green, and the gastroduodenal artery is yellow.

Case 2
This is the next angiogram done on this patient, also normal.
Question 8:
a) What is this vessel?
This is the superior mesenteric artery.
b) What part of the body does it supply?
The superior mesenteric artery supplies the midgut (from mid-duodenum to the middle of the transverse colon.
c) How does the branching pattern of this vessel differ from the celiac artery?
The celiac artery is a very short trunk that immediately divides into two major branches (to the right toward the liver and left toward the spleen) with a smaller branch (the left gastric artery). The superior mesenteric artery has a long main channel that arches out and then down, running parallel to and anterior to the aorta, and giving off many many branches.
d) What is the 'other vessel' you can see by clicking the link below, and what part of the body does it supply?
The 'other vessel' is the inferior mesenteric artery, a much smaller branch than the celiac or superior mesenteric. It supplies the hindgut, from mid-transverse colon to rectum.
Case 2
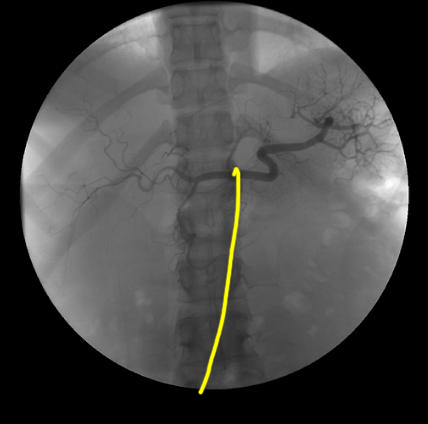
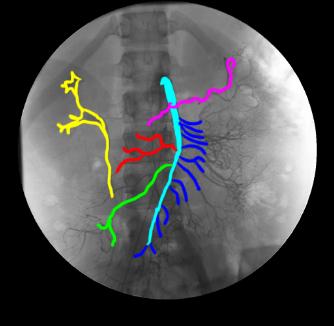
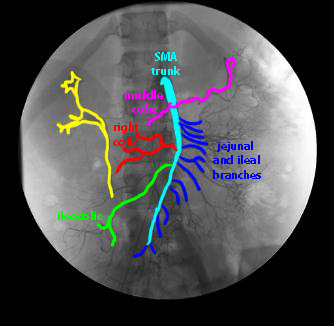
This is a labeled image from the SMA arteriogram. Try to identify branches before clicking on the answer. Then click on the IMA branches link to test your knowledge of these branches as well.
Question 9:
What is indicated in yellow on the labeled SMA arteriogram?
This is the right renal collecting system and ureter. They are visible because the body is beginning to eliminate the contrast material from the blood, and filter it into the urine, making it appear dark on this inverted image.
Case 2
This is part of an angiographic study of a different patient who was an alcoholic who had developed hematemesis.
Question 10:
a) What is this study?
This is a study to look at the portal venous system. The only relatively easy way to get contrast into these vessels is by injecting into one of the arteries that supply the GI tract (celiac, SMA, IMA) and waiting for the contrast to circulate out through the tubular viscera/liver/spleen and back to the portal system.
b) Why is this contrast fainter and less clear than what was seen in the previous arteriograms?
Because there is no easy way to put a catheter directly into the portal system, the contrast has time to become diluted (with unopacified blood) and also to be filtered out by the kidneys.
Click on the labels link below to try identifying the vessels that are visible.

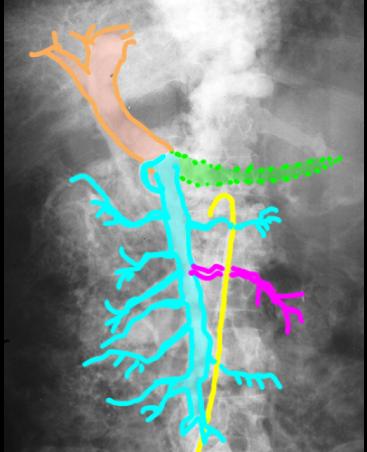
Case 2
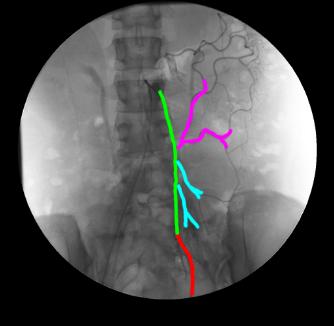
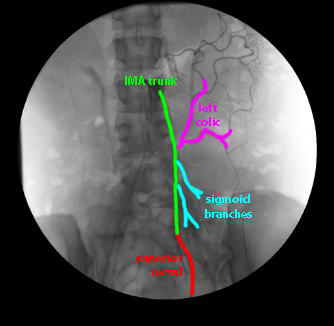
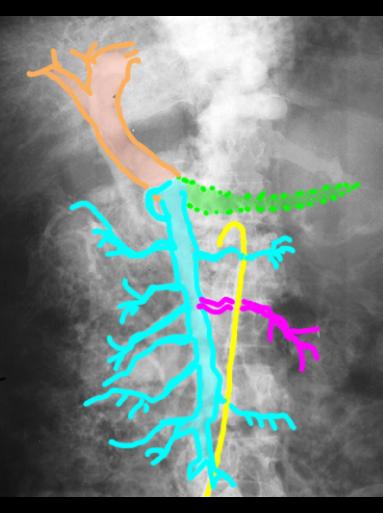
Here is the labeled image from the portal venogram previously shown. Click below to see answers and a mystery.
Question 11:
a) What is indicated in red (mystery) below?
These are tortuous (winding and twisting) enlarged veins from the region of the stomach upward toward the esophagus. Enlarged veins are called varices.
b) How does this relate to the patient's history (alcoholic with hematemesis--vomiting of blood)?
When the liver becomes cirrhotic (scarred), as often happens in alcoholics, the flow in the portal system is blocked as the liver function decreases. The blood coming back from the GI tract has to go somewhere. One of the places it can go is into the veins that connect the upper stomach to the lower esophagus, since the esophageal veins can drain into the mediastinum and vena cavae. Since these dilated varices are just under the mucosa of the esophagus, they can be damaged by passing food and can bleed into the esophagus, leading to hematemesis. Because of the size of the varices, patients may easily bleed to death if treatment is not initiated promptly.
c) What is indicated on the image in yellow?
The yellow label shows the catheter that was used to do the initial angiogram, coming in from the region of the right femoral artery. The catheter tip location suggests that contrast was injected into the SMA to produce this image, after sufficient delay for the contrast to reach the portal system.