Case 4
This is a 65 year old alcoholic male who has increasing abdominal girth.
Question 1:
a) What is this study (be specific)?
This is an abdominal CT scan, axial plane, soft tissue windows, with oral and intravenous contrast.
b) What is one abnormal finding?
There is material in the peritoneal cavity that is intermediate in density between fat and muscle. This is most consistent with something close to water in density. In the setting of alcoholic liver disease, this is likely ascites, or fluid in the peritoneal cavity, and accounts for increasing girth.
Case 4
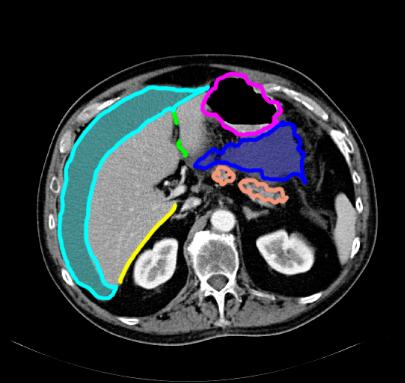
This is a selected image from the prior CT study. The link below shows structures on this slice for you to identify.
Question 2:
How can you tell that this is a CT and not an MR?
Bones are white. In fact, it is hard to see any cortex vs medulla in any of the bones, indicating that this is not displayed with a BONE window. On MRI, cortical bone is always dark. Medullary bone may be bright, depending on the particular sequence being performed, but the outer rim of dense cortical bone should always be dark.
Try to identify the outlined structures on this image before moving on to the next image.

Case 4
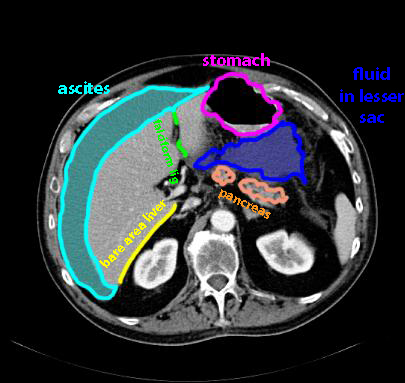
These are the structures previously labeled.
Question 3:
a) What segments of the liver does the falciform ligament separate?
The falciform ligament divides the medial and lateral segments of the left lobe of the liver, from the clinical point of view based on vascular supply. The classic anatomic organization of the liver divides the right lobe from left lobe at the falciform ligament.
b) What is the lesser sac?
The lesser sac is a protrusion of the peritoneal cavity (the greater sac) into the space between the back wall of the stomach and the front surface of the pancreas. The region of the connection between the lesser and greater sacs is the foramen of Winslow (epiploic foramen), located near the aorta hepatis ('door' to the liver).
c) What is the bare area of the liver?
The surface of the liver is almost all covered by visceral peritoneum, which reflects back along the inner abdominal wall as parietal peritoneum, enclosing the greater sac (peritoneal cavity). There is a triangular superior-posterior portion of the liver that is not covered by peritoneum, which is the bare area. It can be seen on this CT because the ascites fluid cannot wrap around in back, but ends where it reaches the lateral margin of the bare area.
Case 4
This study is from a different patient with similar history, a 64 year old female alcoholic with increasing girth.
Question 4:
a) What type of study is this? (Be specific)
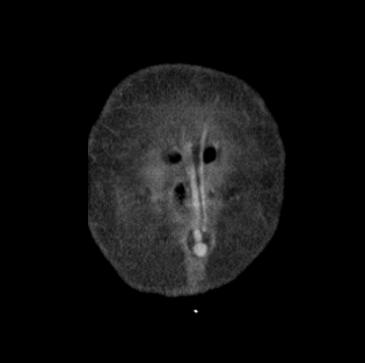
This is a CT scan reconstructed in the coronal plane, with oral and IV contrast, displayed in soft tissue windows.
b) Do you see anything unusual on the slices through the anterior abdominal wall?
There is a tubular structure that seems to connect to the region of the umbilicus, that looks like it is filled with IV contrast, consistent with an abnormal dilated vessel.
Case 4
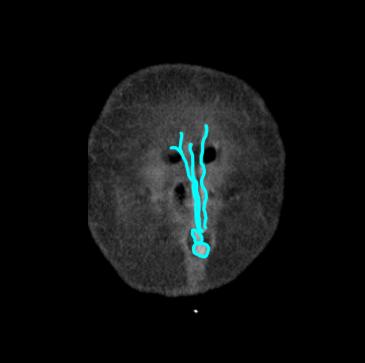
The abnormal vessel is shown below. Try to follow its course back from the anterior body wall on the provided images.
Question 5:
a) What does this vessel connect to?
It connects to the region of the falciform ligament and then into the portal vein.
b) What would such a vessel look like on physical exam of this patient?
It would be a dilated tortuous (twisting) vessel just visible under the surface of the skin, radiating out from the umbilicus. This appearance is called a 'caput medusae' (head of Medusa).
c) What is the significance of this finding in a patient with alcoholic liver disease and ascites?
The finding of dilated vessels in the region of the umbilicus connecting to the portal system are a sign of portal hypertension, often due to cirrhosis of the liver. When the liver becomes hard and scarred, flow in the portal vein can become blocked. Blood trying to return from the GI tract seeks alternate routes to detour around the liver. Some patients develop esophageal varices (as were seen in a previous case) and others develop hemorrhoids. And some patients develop channels out along the falciform ligament to the anterior body wall in the region of the umbilicus. These are due to recanalization of the fetal circulatory path whereby oxygenated placental blood from the mother entered the fetal circulation via the umbilical cord, flowing into the portal vein in the region of the falciform ligament.