Case 1
This 82 year old female had sudden onset of severe abdominal pain and bloating.
Question 1:
a) What is this study? Be specific.
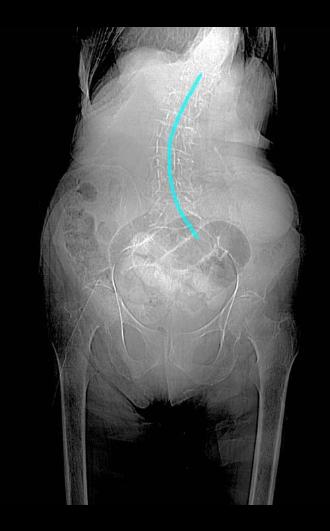
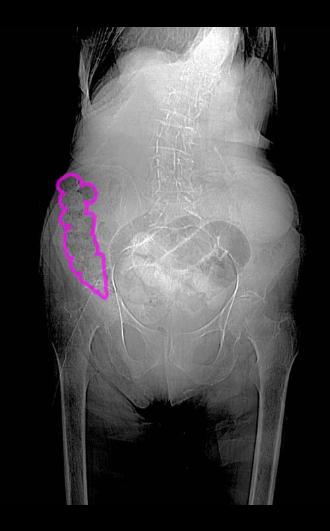
This is definitely a projection image. But it is not a typical abdominal radiograph because the area shown (from mid lungs to mid-thighs) is too large for any standard radiographic image. It is a scout image (topogram, scanogram) for planning a CT study. It is a low resolution type of abdominal radiograph done on the CT table to show the technologist where to start and stop the scan.
b) What do you think of the patient's bones?
The bones look very washed out. Even the iliac crests, which are usually easy to see, are very faint. This suggests that the patient is severely osteopenia (has lost bone density). Also, there is fairly severe curvature of the lumbar spine in the coronal plane, called scoliosis.

Case 1
This is the same CT scout image shown previously. While it is not of the same quality as a real abdominal radiograph (often termed a 'KUB' for 'kidney, ureter, bladder), it can still show some findings, as noted including osteopenia and scoliosis. Click on the link below for 'spine' to check the degree of curvature.
Question 2:
a) What part of the GI track is outlined below as 'bowel 1', and does it look normal?
Bowel 1 is small bowel, based on its 'back and forth' or stacked loop appearance. The loops are dilated with too much gas for normal small bowel, which usually contains mostly fluid. Fluid-filled bowel loops are invisible on abdominal radiographs, since they blend with all the other soft tissues in the abdomen.
b) What part of the GI track is outlined below as 'bowel 2', and does it look normal?
Bowel 2 is part of the colon, based on its peripheral location and the speckled appearance of its contents. This is the typical appearance of stool on abdominal radiography. This is most likely the ascending colon and appears normal.


Case 1
This is a normal radiograph of the pelvis in a different patient. You can flip back and forth between this image and our patient's image to see how different the normally mineralized bones look, compared to the osteopenia in our patient.
Question 3:
a) What bony structure is outlined on our patient's image (click the link below for 'patient and structure')?
The purple outline shows the obturator foramen.
b) What goes through the opening outlined on our patient's image?
Most of the obturator foramen is covered by the densely fibrotic obturator membrane, providing attachment for muscles of the pelvic wall. Only a very tiny opening is left in the upper anterior part of the large bony foramen, through which the obturator nerve, artery and vein pass.


Case 1
This is the normal pelvic radiograph shown again, with links to several structures for you to identify.
Question 4:
a) How would you describe the projection for this radiograph?
In almost all parts of the body except the chest, we typically do a front-wise view of the area of interest with the beam passing from the patients anterior surface toward the posterior, or AP view. We do a PA view for the chest only specifically so that there will be no artificial magnification of the heart on the final image. So this pelvis radiograph was done AP.
b) What muscles attach to the foramen outlined below?
This is again the obturator foramen. On the inside, the obturator internus muscle attaches, and on the outside, the obturator externus attaches.
c) What are bony structures 1 and 2 indicated below?
Bony structure 1 is the superior pubic ramus, forming the upper margin of the obturator foramen. Bony structure 2 is the ischial tuberosity.
d) What are listed as 'structures to identify'?
The two bony surfaces are the pubic bones, which come together anteriorly in the midline to form the pubic symphysis, a special firm type of joint that allows very little motion. The gap between the two bones is filled with hyaline and fibrocartilage.






Case 1
This is an imaging study on a different patient with chronic right hip pain. Selected images are shown in the region of the obturator foramen.
Question 5:
a) What type of study is this? Be specific.
This is an axial CT scan displayed with soft tissue windows, with IV contrast.
b) On the link below (labels), what is outlined in purple?
The obturator internus muscle is outlined in purple, lining the inside of the obturator foramen.
c) On the labeled images, what is outlined in yellow?
The obturator externus muscle is outlined in yellow, lining the outside of the obturator foramen.
d) On the labeled images, what is outlined in red and blue?
The obturator artery and vein are outlined in red and blue. On the top image, they are just passing through the upper anterior gap in the obturator membrane, and on the lowest slice, they are passing anterior to the obturator externus muscle to reach the inner thigh (adductor) muscles.
Case 1
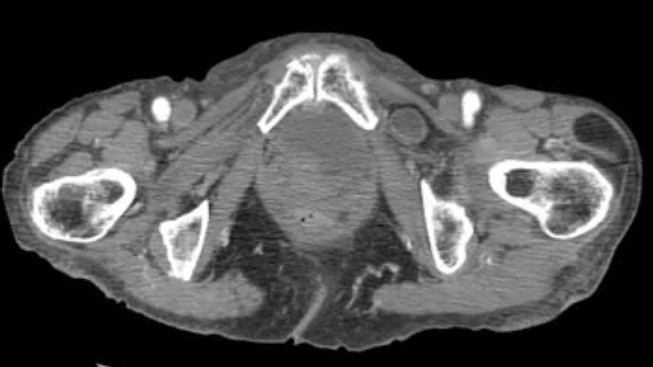
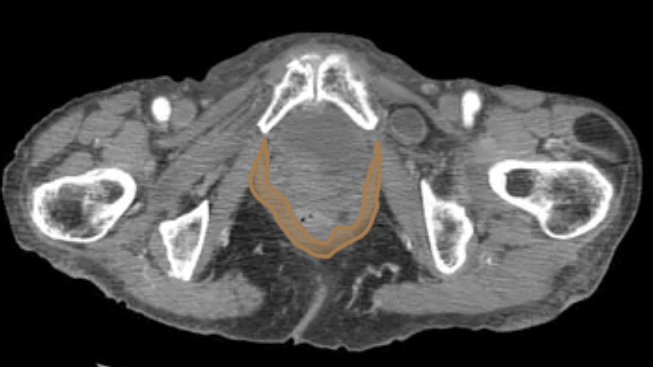
This is the CT scan of our patient, whose topogram we reviewed earlier, showing scoliosis, osteopenia, and some dilated mid-abdominal small bowel loops. A red asterisk has been placed on a small bowel loop in the left lower quadrant of her abdomen. Try to trace the course of this loop through the scan images.
Question 6:
What is abnormal about the course of the indicated small bowel loop?
If you follow it carefully, you can see that it passes out through the obturator foramen, in the region where normally only the obturator nerve and vessels exit. This is called an obturator hernia.
Case 1
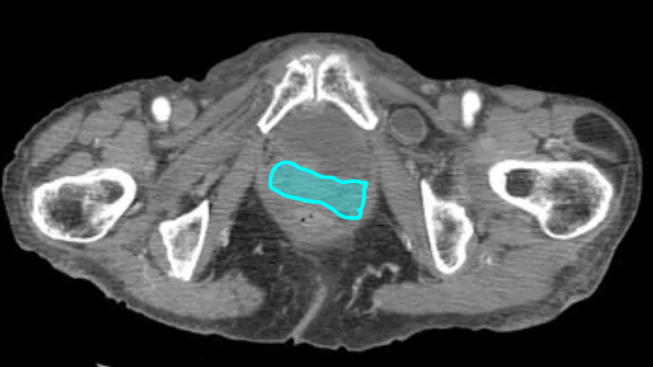
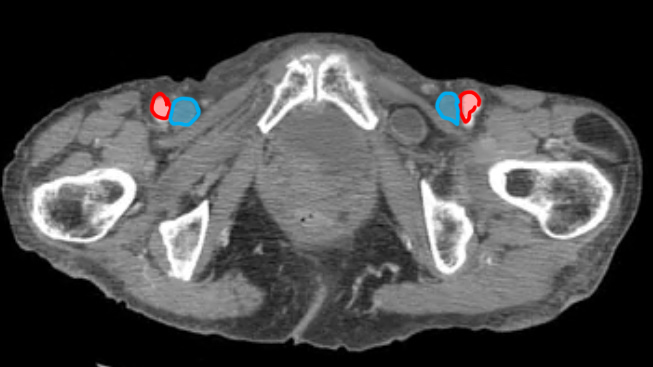
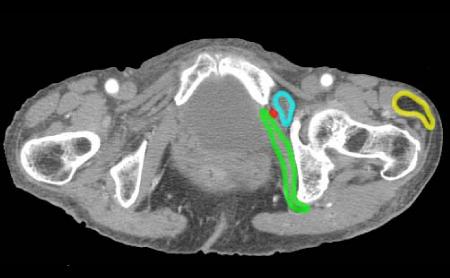
This is a selected image from our patient's CT scan showing the left obturator hernia in blue.
Question 7:
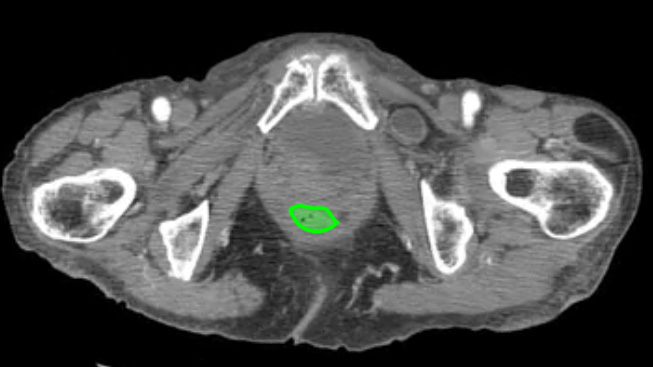
a) What is indicated in green and red?
The green outline indicates the obturator internus muscle, and the red dot is the obturator artery.
b) This hernia is quite small. Does that mean it is not clinically significant?
In fact, smaller hernias, particularly if they are passing through a small tight opening (like this one is) are the MOST worrisome. They are prone to compromising their blood supply due to the tightness to the opening through which they pass. Larger hernias are presumably passing through a large, more lax opening and should not become ischemic (loss of blood supply) as easily. This small bowel loop was already necrotic by the time this patient went from CT to the OR. She required resection of several feet of small bowel.
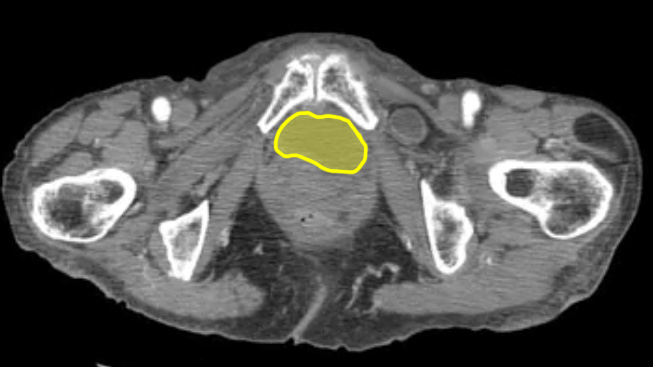
c) What density is the area outlined in yellow?
This has a density similar to subcutaneous fat. It is an incidental benign fatty tumor called a lipoma. Lipomas are very common and generally need no treatment.
Case 1
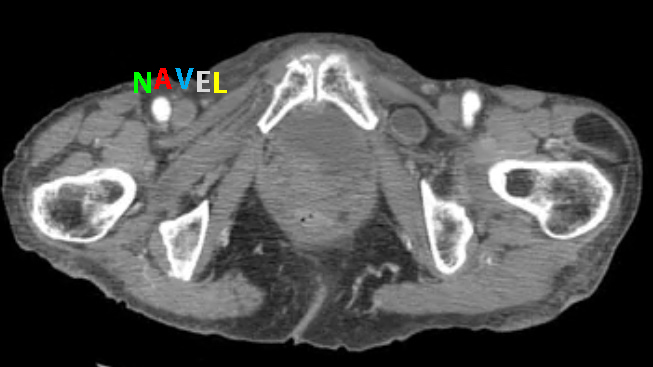
This is the lowest cut from the patient's CT scan
Question 8:
a) Try to identify the structures indicated below before clicking the links. Why is the density of the femoral artery so different from that of the femoral vein?
This has to do with the timing of scanning after IV contrast administration. Scanning can begin very early (if the clinical question has to do with upper body VEINS), a bit later (if the question has to do with pulmonary embolism), a bit later (if the question relates to the aorta or its branches), or even later (at what is called the equilibrium phase), where arteries and veins show similar contrast density throughout the body. This scan was done in the arterial phase, so the femoral artery is very bright, but the contrast has not yet reached the femoral vein.
b) Why is the relationship of the femoral artery to the vein of clinical importance?
The mnemonic shown below is useful to remind you that the femoral artery is LATERAL to the femoral vein. This is of major importance in the acute setting where sometimes a CVL must be quickly placed into the femoral vein to administer large volumes of fluids, blood or medications quickly. You can generally feel the femoral pulse, so you know to place your catheter MEDIAL to the pulse, if you do not have access to an ultrasound to guide you.