Case 4
This study is from a 50 year old woman with abdominal fullness, pelvic pain and heavy menses for many years.
Question 1:
a) What type of study is this? Be specific.
This is an MRI (cortical bone is dark), in the sagittal plane with T2 weighting (water, such as the urine in the bladder is bright).
b) Is fat ever bright on CT?
No. But fat is not always bright on MR, so it if you do see bright fat you know it is an MR, but if you see dark fat, it could either be a CT or an MR with fat saturation (fat suppression).
Case 4
This is a section near the midline from this patient's MRI study for you to look again for cortical bone, fat and fluid.
Question 2:
a) How does the radiation for an MRI compare to that of a CT scan?
There is no radiation from an MRI. There is a relatively high dose of radiation from a CT scan.
b) Are there any contraindications to MRI?
The commonest reason that a person cannot have an MRI is actually claustrophobia. Some patients can manage with mild sedation but others cannot. Other contraindications are metal fragments in the eye, pacemakers or other types of electronic implanted devices. Inability to hold still for up to an hour is not really a contraindication, but can result in images with limited diagnostic value due to motion. Some older surgical clips can be a contraindication.




Case 4
This is the same mid-sagittal T2-weighted MR image.
Question 3:
a) How could you tell a fluid pocket from fat on this image?
It is difficult to tell fluid from fat on a T2-weighted image with bright fat. That is why we often do T2-weighted images with fat suppression (fat saturation). If you turn down the signal from fat, only fluid will be bright.
b) Is fluid increased in areas of pathology?
Yes. If you think of all different kinds of abnormalities, most often they will have increased fluid, whether it is infection, trauma, tumor, or inflammation. So a T2-weighted sequence with fat suppression is an excellent way to look at pathology.
c) Why might you do T1-weighted imaging without fat saturation?
In T1-weighted images without fat saturation, fat is the only bright thing on the image. It usually outlines all of the interesting and important anatomic structures, like organs, muscles, etc. So a T1-weighted image with bright fat is an excellent sequence to look at anatomy.

Case 4
This is again the midline sagittal view of the patient's MRI. Try to identify the listed structures before clicking on their links.
Question 4:
a) Does the scan time change when you do both T1 and T2 weighted sequences?
Yes. Unlike CT (where you can change windows and imaging planes after the patient has left the department), for MR, each imaging plane and each sequence setting (like T1, T2, fat suppression) requires a new scan with the patient in the magnet. Most MR imaging takes far longer than even the most complicated CT scan.
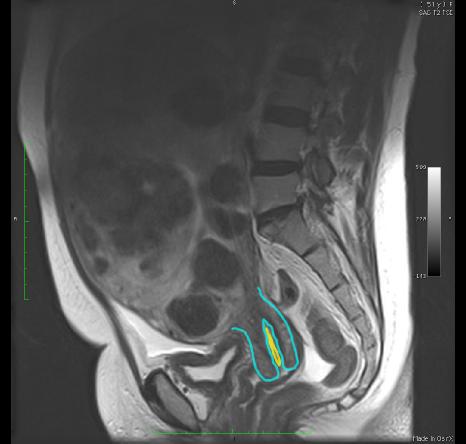
b) Where is there fluid on these T2-weighted images besides in the bladder and CSF space of the sacrum?
There is trace of fluid in the cervical canal and in the vagina, as indicated below in yellow.





Case 4
This is the same midline sagittal image in our patient. Recall that her symptoms were abdominal fullness and heavy menses. What do you think of her uterus?
Question 5:
a) If you click on 'abnormality' below, you will see the uterus. How would you describe this appearance?
This uterus is very heterogeneous in signal, containing many rounded masses. It is also hugely enlarged, about the size of a late term pregnancy.
b) Can you think of any common condition that could produce this appearance?
Many rounded masses in the uterus is most consistent with fibroids, which can be multiple and large, and can produce heavy menses. This patient was actually anemic from all of her blood loss on a monthly basis.


Case 4
This is another set of images on the same patient, limited to the lowermost part of the pelvis.
Question 6:
What type of images are these? Be specific.
Since bones are not very visible (being dark overall), this is an MRI. Images were obtained in the axial plane. There is no fat suppression, as fat is bright. Urine in the bladder is dark, so this is a T1-weighted sequence.
Case 4
This is the same set of T1-weighted axial lower pelvic images. Try to identify the labeled structures.
Question 7:
a) What passes through the greater sciatic foramen?
The largest thing is the pyriformis muscle. The pudendal (and its accompanying vessels) and sciatic nerves also pass out from the pelvis to the gluteal region. The superior gluteal vessels pass out superior to pyriformis and the inferior gluteal vessels pass out inferior to pyriformis. There are also several smaller nerves that pass through going to specific muscles: nerve to quadratus femoris, superior and inferior gluteal nerves, and the nerve to obturator internus. The posterior femoral cutaneous nerve also exits here to reach the back of the thigh.
b) What passes through the lesser sciatic foramen?
After exiting the pelvis via the greater sciatic foramen, the pudendal nerve (and accomanying vessels) return the the perineum through the lesser sciatic foramen. The tendon of obturator internus makes its way to the femur through the lesser sciatic foramen, along with the nerve to obturator internus (which exited via the greater sciatic foramen originally).
Case 4
This is the same set of labeled axial T1-weighted MR images of the lower pelvis.
Further Explanation:
The openings of the posterior pelvis (the greater and lesser sciatic foramena) are illustrated on these labeled images. The bony margin of the greater sciatic notch is outlined in dark blue. The pyriformis muscle, which is the largest structure passing through the greater sciatic foramen, is indicated in pink. The greater and lesser sciatic notches become foramena through the contribution of ligaments, the sacrotuberous (indicated in orange) and sacrospinous (indicated in yellow). These ligaments pass from the sacrum to the ischial tuberosity (light blue) and the ischial spine (light green). The course of the pudendal nerve and its accompanying internal pudendal vessels is shown in purple. This neurovascular bundle exits through the greater sciatic foramen into the gluteal region, but then passes anteriorly through the lesser sciatic foramen to reach the perineum from posteriorly.
Case 4
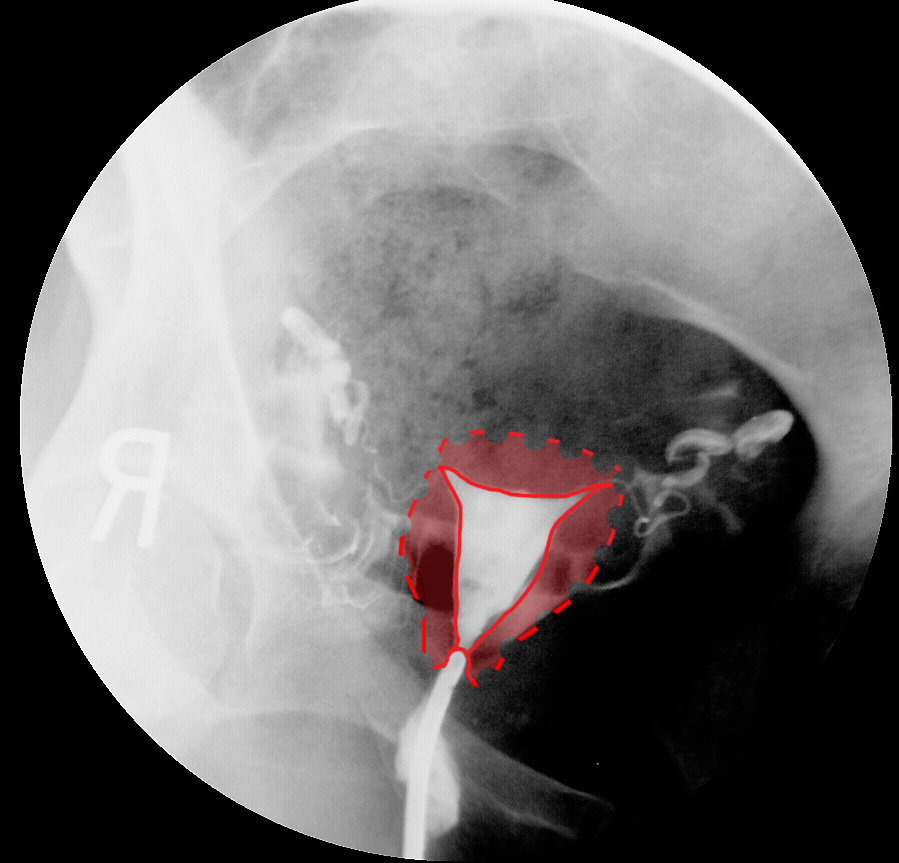
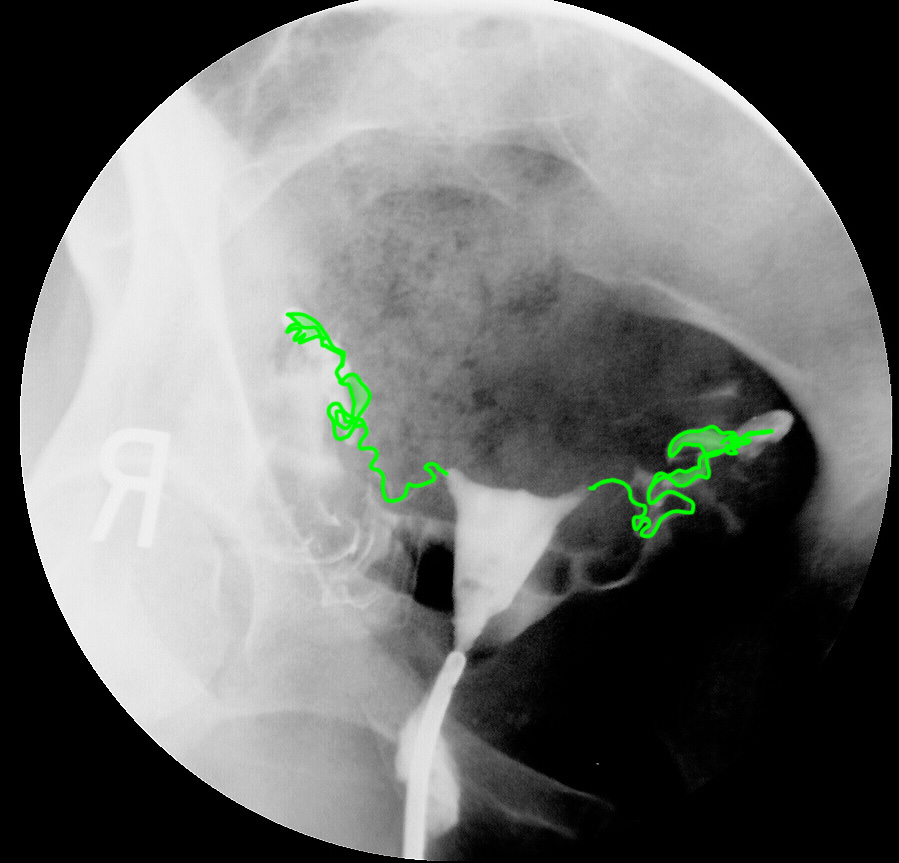
This is a 25 year old patient with a complaint of infertility. Try to identify the indicated structures before clicking the links below.
Question 8:
a) What is shown on this study?
This is a study called a hysterosalpingogram. Contrast is injected into the lumen of the uterus to show its shape. Contrast should normally pass into the thin, tortuous uterine tubes, and then out into the peritoneal cavity.
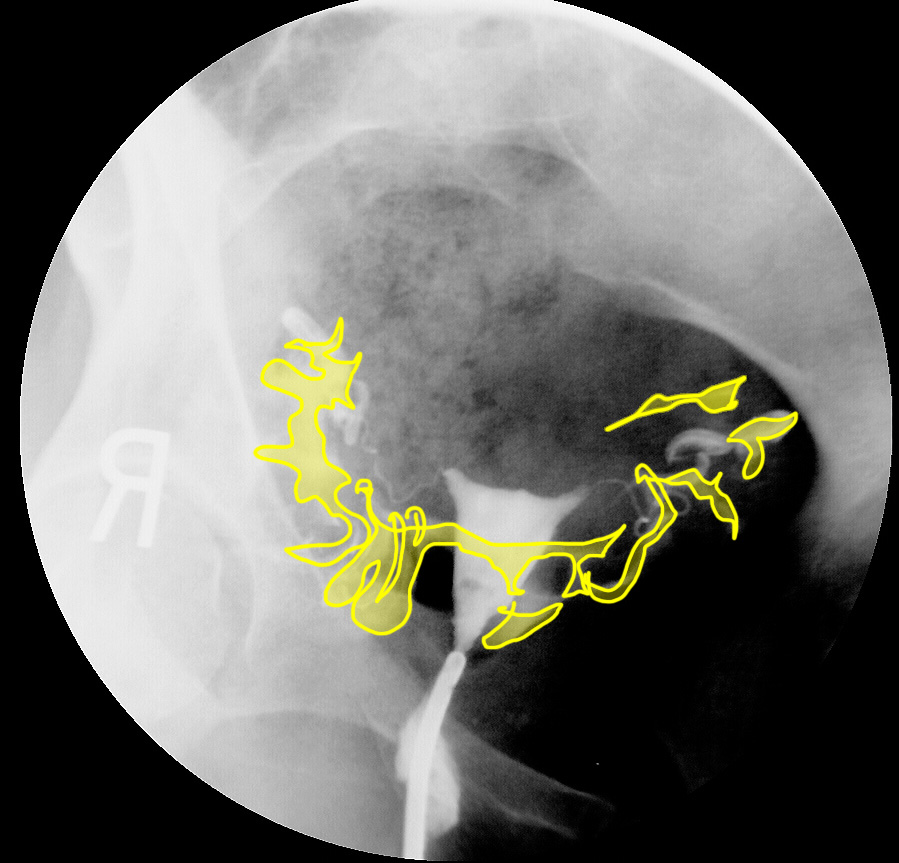
b) What is the mystery link below?
The mystery link shows the appearance of contrast that has entered the peritoneal cavity (through the fimbriated ends of the uterine tubes). This is normal, and indicates that the patient's infertility is not due to blockage somewhere along the system. It is normal for the uterine tubes to open into the peritoneal cavity. Faint outlines of small bowel loops can be seen with contrast outside of them.