













Case 1
This is a 60 year old male with chronic left flank pain and intermittent microscopic hematuria.
Question 1:
a) What is this study. Be specific.
This is an abdominal radiograph, also called a KUB (for kidneys, ureters and bladder). The patient position is usually supine unless a different position is requested (such as prone, decubitus or upright).
b) Was IV contrast given?
Your initial thought may be 'yes' as it looks like we are seeing the left renal calyces and renal pelvis. However there is no contrast beyond this and there is abrupt cutoff of the dense appearing material in the renal pelvis area. There is also no hint of contrast in the renal parenchyma. This is a large renal stone, called a 'stag horn' calculus because of its shape. It forms when solutes precipitate out of the urine, most often in the setting of chronic infection where bacteria can alter urine pH, leading to in situ stone formation within the collecting system.
c) What is mystery 1 (label indicated below)?
Mystery 1 shows some fairly large calcifications located very low in the pelvis, overlying the pubic symphysis. These are common findings in the prostate gland and are not of clinical significance.
d) What is mystery 2?
Mystery 2 shows a smooth rounded soft tissue density in the pelvis most consistent with a bladder full of urine. While small water-density areas on a KUB are not usually visible, if you get enough water in a spherical collection like this, it can be faintly seen due to summation as the beam passes through. This might suggest an bladder outlet obstruction, which might commonly be due to an enlarged prostate in a patient of this age.
e) What is mystery 3?
Mystery 3 shows a smooth rounded calcification higher in the left side of the pelvis. It seems a bit lower than the distal ureter location, so it is more likely another common incidental benign calcification in the pelvis called a phlebolith (vein stone). These occur due to sluggish flow in various pelvic veins often adjacent to the bladder, resulting in chronic clots that eventually calcify.




Case 1
This is a study from a 25 year old man with acute right severe flank pain and hematuria.
Question 2:
a) What is this study? Be specific.
This is a CT scan in the axial plane without oral or intravenous contrast, displayed with soft tissue windows.
b) What diagnosis is suggested by the patient's clinical presentation?
Acute severe flank pain and hematuria are very suggestive of a renal stone.
c) Is there another thing that could be done at the time of this study to maximize visualization of findings in this setting?
If renal stone is the top diagnosis, the abdominal CT scan is often done in the prone position rather than supine. In this way, if a stone has passed into the bladder, it can be readily identified in an anterior location (in the prone position). In the supine position, bladder stones and distal ureteral stones can be hard to tell apart, as both will be posterior in location.
Case 1
These are selected images from the same CT previously shown.
Question 3:
a) Where do you think the calcification is located on this image?
A tiny fleck of calcium is present in the prostate, a common benign and incidental finding.
b) Where is the calcification located on slice 2?
A tiny calcification is present in the distal-most right ureter, near the wall of the bladder. The right ureter appears minimally more dilated than the left ureter on this image.
c) Where is the calcification located on slice 3?
There is a VERY tiny calcification in the right kidney, and the right collecting system appears more dilated than the left kidney, consistent with obstruction from the distal right ureteral stone.


Case 1
This is a 65 year old male with history of multiple episodes of right renal colic in the past and intermittent hematuria.
Question 4:
a) What is this study, and which is the superior part of the patient?
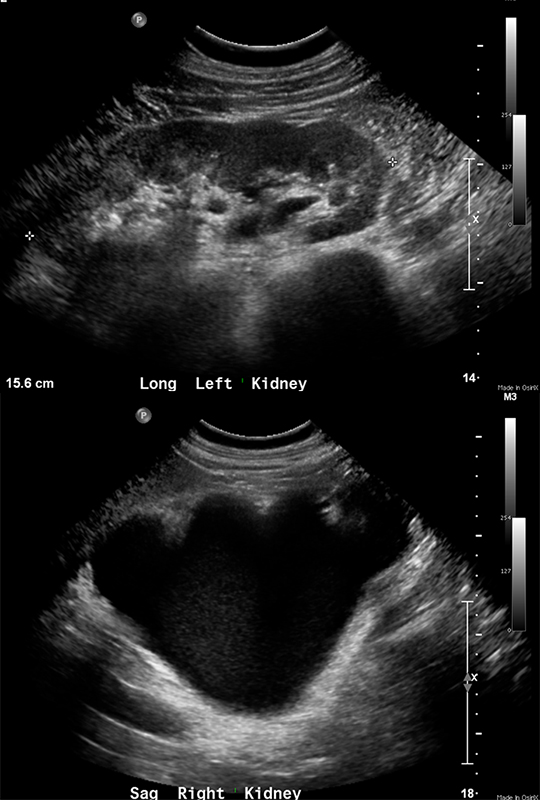
This is a renal ultrasound, and the patient's head is to the left side of the image.
b) What is abnormal?
The right collecting system is very dilated, so there is likely some point of obstruction below the level of the renal pelvis. Sometimes a dilated ureter can be found and followed on ultrasound, but it depends on how much bowel gas is interfering with imaging. In this patient, the ureter could not be seen well with ultrasound.
c) What would you do next?
A reason for the right hydronephrosis (dilated collecting system) must be sought, so CT is the next study to do.
Case 1
This is the CT on the same patient as the prior ultrasound.
Question 5:
a) What are imaging parameters, and are they ideal for detection of renal stones?
This is a coronal reformatted CT series with oral and intravenous contrast and supine positioning. These are not the ideal parameters for detection of renal stones, which should be without oral or intravenous contrast, and with the patient in the prone position. You can see from the first image of the series that the patient was in the supine position, as you can see the support couch behind the posterior part of his body.
b) What is abnormal?
The right kidney is just a huge dilated fluid filled collecting system with little remaining parenchyma, consistent with atrophy due to long-standing obstruction. No obvious right stone is evident. There is a stone in the left kidney but the left collecting system is not dilated. It is possible that a previous right stone led to the obstruction, but was later passed or surgically removed.
Case 1
This is a 40 year old female with severe right flank pain after a recent hysterectomy.
Question 6:
a) What are imaging parameters for this exam?
This is an axial CT shown with soft tissue windows, and with both oral and intravenous contrast.
b) What do you think of the kidneys and ureters?
There is dilation of the right collecting system and ureter, which continues down to the final cut where a very bright object is seen. It is so dense that it has a star artifact, indicating it is made of metal. This is a surgical clip. Accidental obstruction of the ureter is a known complication of pelvic surgery, since the ureter runs very close to many other vascular structures, in particular the internal iliac vessels.
Case 1
This is another patient with vague pelvic pain and left flank pain, gradually increasing over time.
Question 7:
a) What are technical parameters for this study?
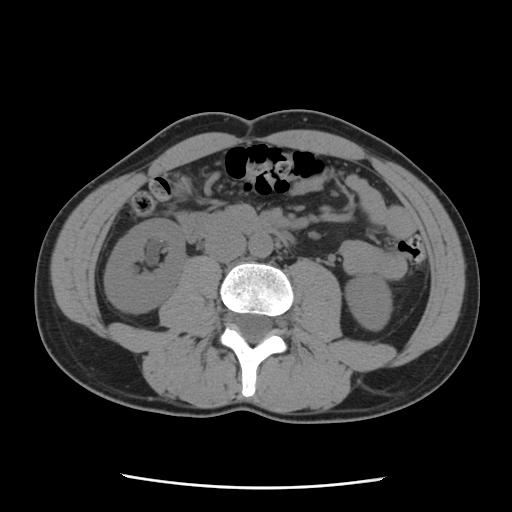
This is a CT scan in the axial plane displayed with soft tissue windows, with both oral and IV contrast. Again, the symptoms were not specific enough to warrant a CT with renal stone protocol, so a more general study was done.
b) What do you think of the kidneys?
There is severe left hydropnehrosis, with dilated ureter extending to the pelvis.
c) What do you think of the bladder?
There is a large irregular mass centered to the left, likely obstructing the distal left ureter. This was found to be a transition cell carcinoma of the bladder, but one could also consider a tumor of the prostate, give the location of the mass.
Case 1
This is a single image from a patient with anemia, peripheral edema, gradual drop in urine output, weakness, and itchy skin. Blood tests showed severely elevated BUN and creatinine (indicating compromised renal function).
Question 8:
a) What are imaging parameters for this study?
This is a CT in the axial plane displayed with soft tissue windows, and with no oral or IV contrast.
b) What do you think of the kidneys?
Both kidneys look very small with thin cortex. There is no evidence of dilated collecting systems on either side, so this atrophy is not likely to be due to obstruction. These kidneys have the appearance of chronic renal disease, which can be from many causes.
c) Do you need to change the CT protocol based on renal function blood tests?
Yes. If the BUN and creatinine (markers of renal function) are elevated, no IV contrast should be given. However, if the patient has such bad renal function that they are already on dialysis, then IV contrast can be given if timed so that it can be quickly removed by dialysis after administration. If the kidneys are already non-functioning, the IV contrast cannot really damage them further.




