Abdomen Pelvis Case 1
The image shown is from a study on a 51 year old patient with vague upper abdominal pain after eating for several months.
Question 1:
a) What is this study and what are pertinent technical parameters to recognize, and why is it important to recognize the window in which an image is displayed?
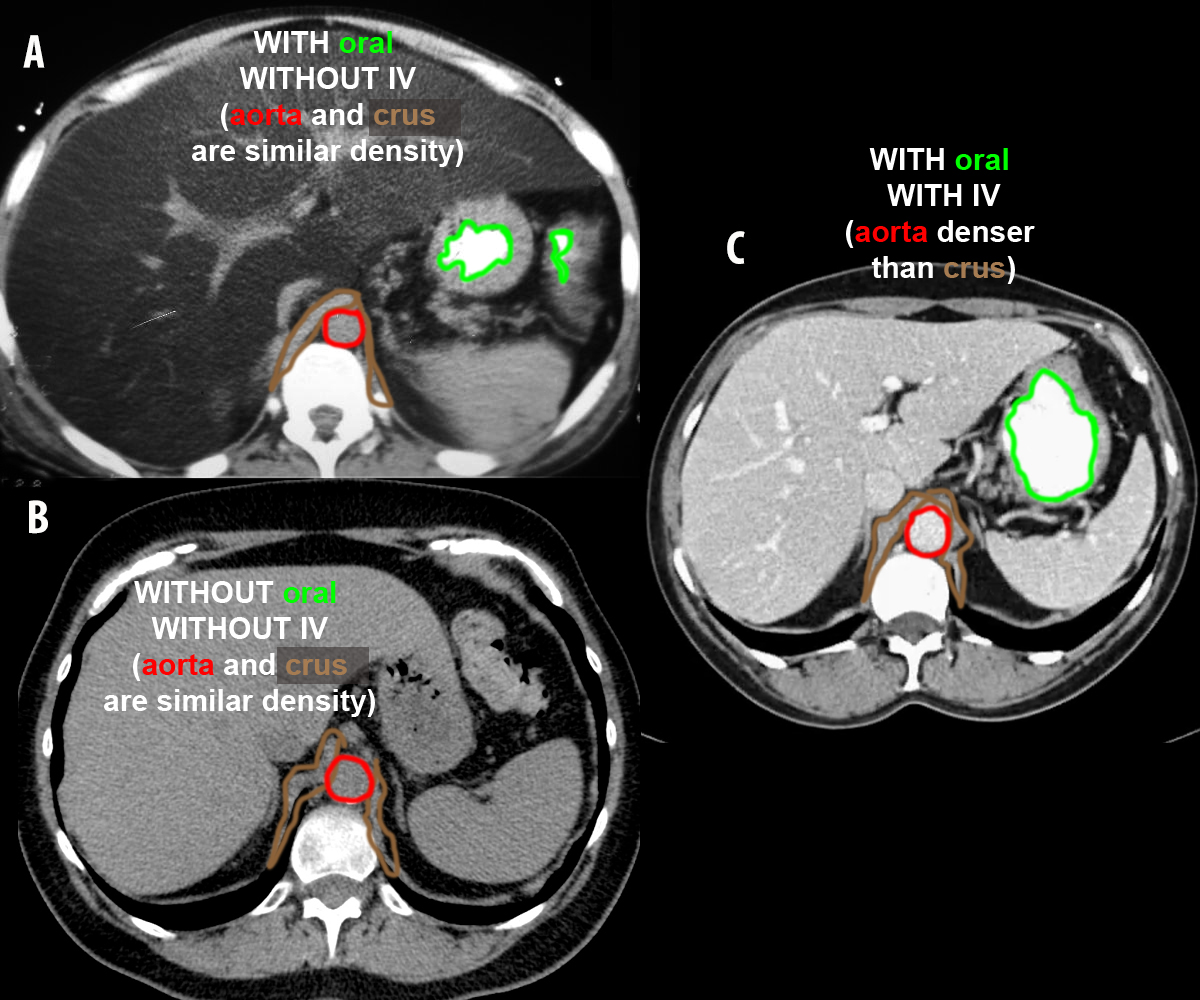
This is axial CT scan of the abdomen displayed with soft tissue windows, with oral but no IV contrast present. Compare the density of the blood in the aorta to the density of any adjacent muscle (the crus of the diaphragm is useful for this in the upper abdomen). Unopacified blood should be the same density as muscle. Click the links below to see these structures outlined. Of course, it is possible that the IV contrast has not yet reached the aorta, but this would be a very unusual timing for abdominal imaging. Early scanning before contrast reaches the aorta is used mostly for either imaging of the upper extremity veins or the pulmonary arteries, but not for the abdominal organs. It is vital to use the right CT window for the structures of interest. You will not see lung disease very well on a soft tissue window. You will not see bony abnormalities very well on a soft tissue window. It will be hard to detect abnormal blood flow on a bone or lung window.
b) How is a CT different from an MR, from the patient's point of view?
An MR is a more enclosed space (so many patients have problems with claustrophobia), and an MR takes much longer to complete than a CT. This is because each separate sequence and imaging plane must be obtained while the patient is in the scanner. They cannot be changed after the fact. For a CT, once the patient data is collected (usually in a few minutes), many of the imaging features can then be changed as needed, including the viewing window and the imaging plane. The presence and timing of oral and IV contrast must be managed at the time of the scan, and cannot be changed afterward.
c) How should liver density compare to spleen density?
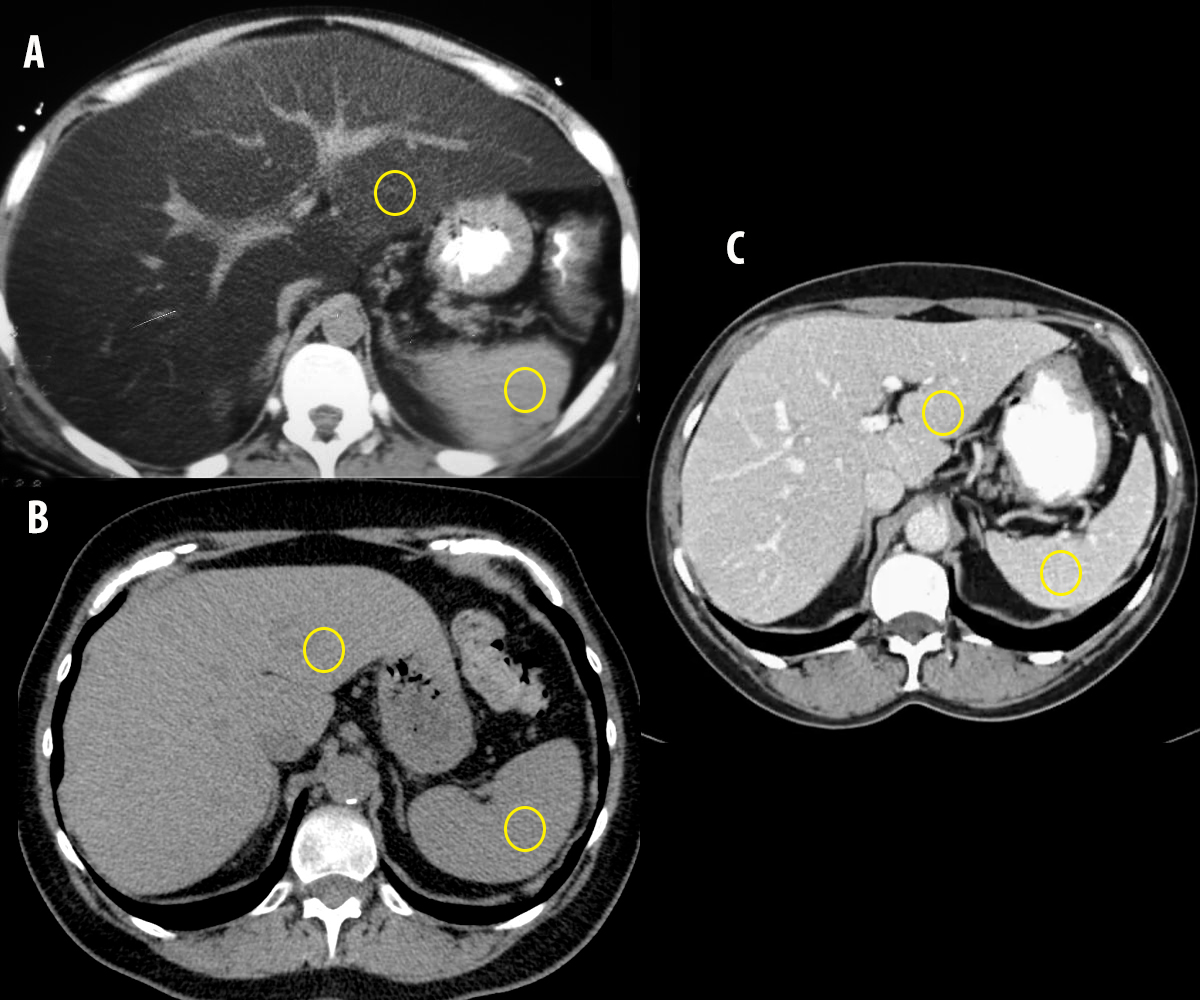
Visually, the liver and the spleen should be similar in density. Look at the 'liver vs spleen density' link to decide which of these three images is ABNORMAL.
Abdomen Pelvis Case 1
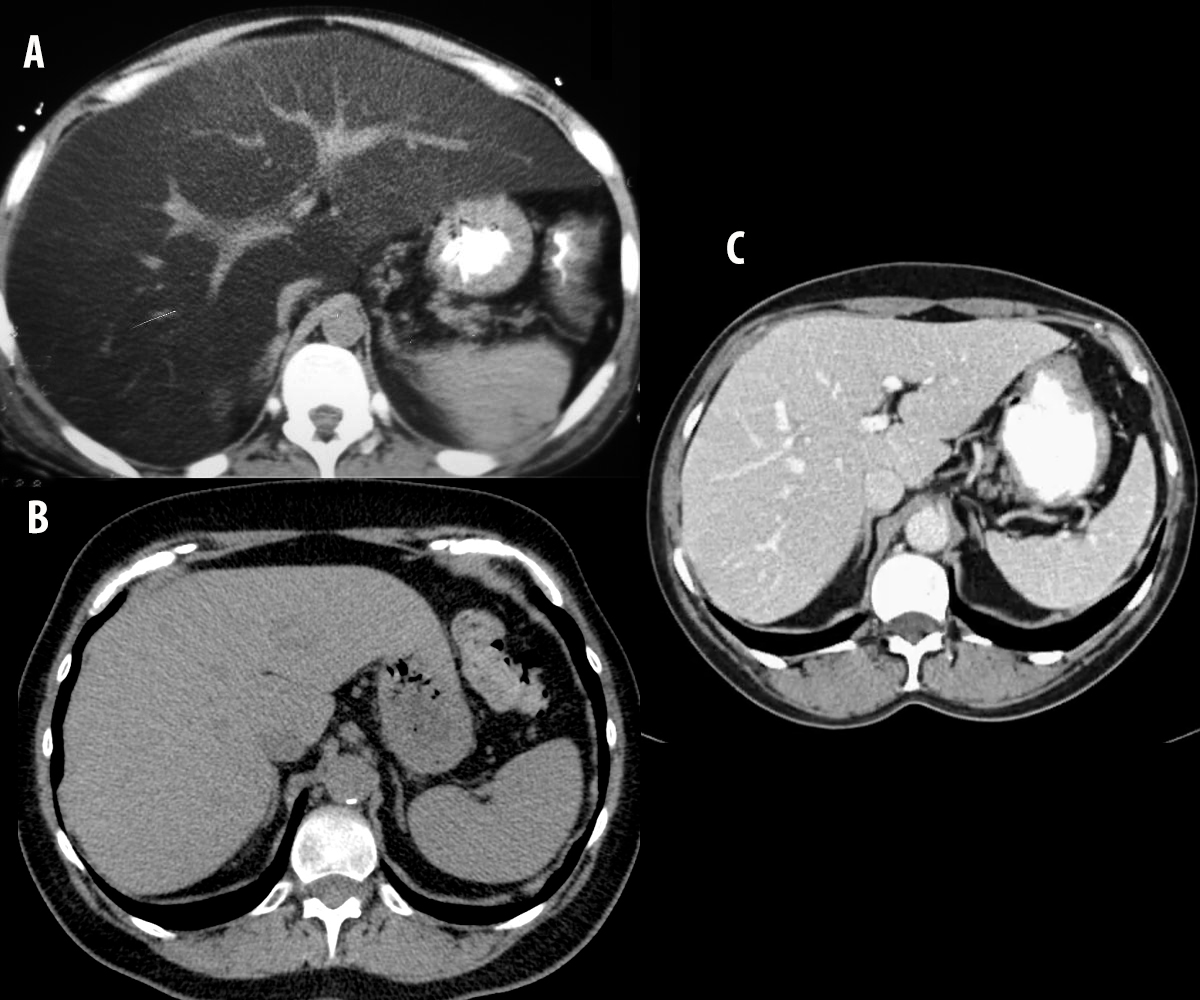
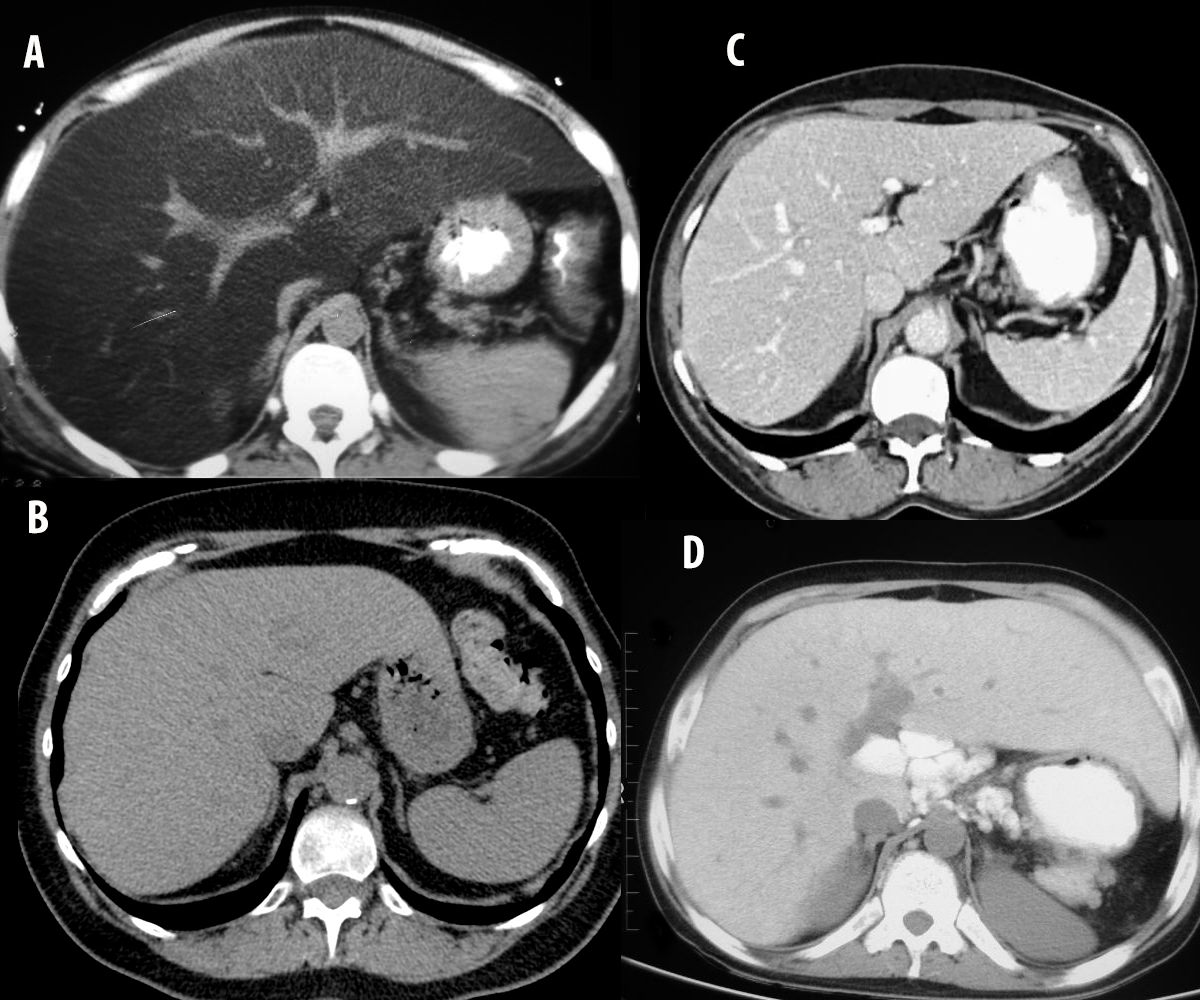
Image A is from the original patient. Images B, C and D are from other patients.
Question 2:
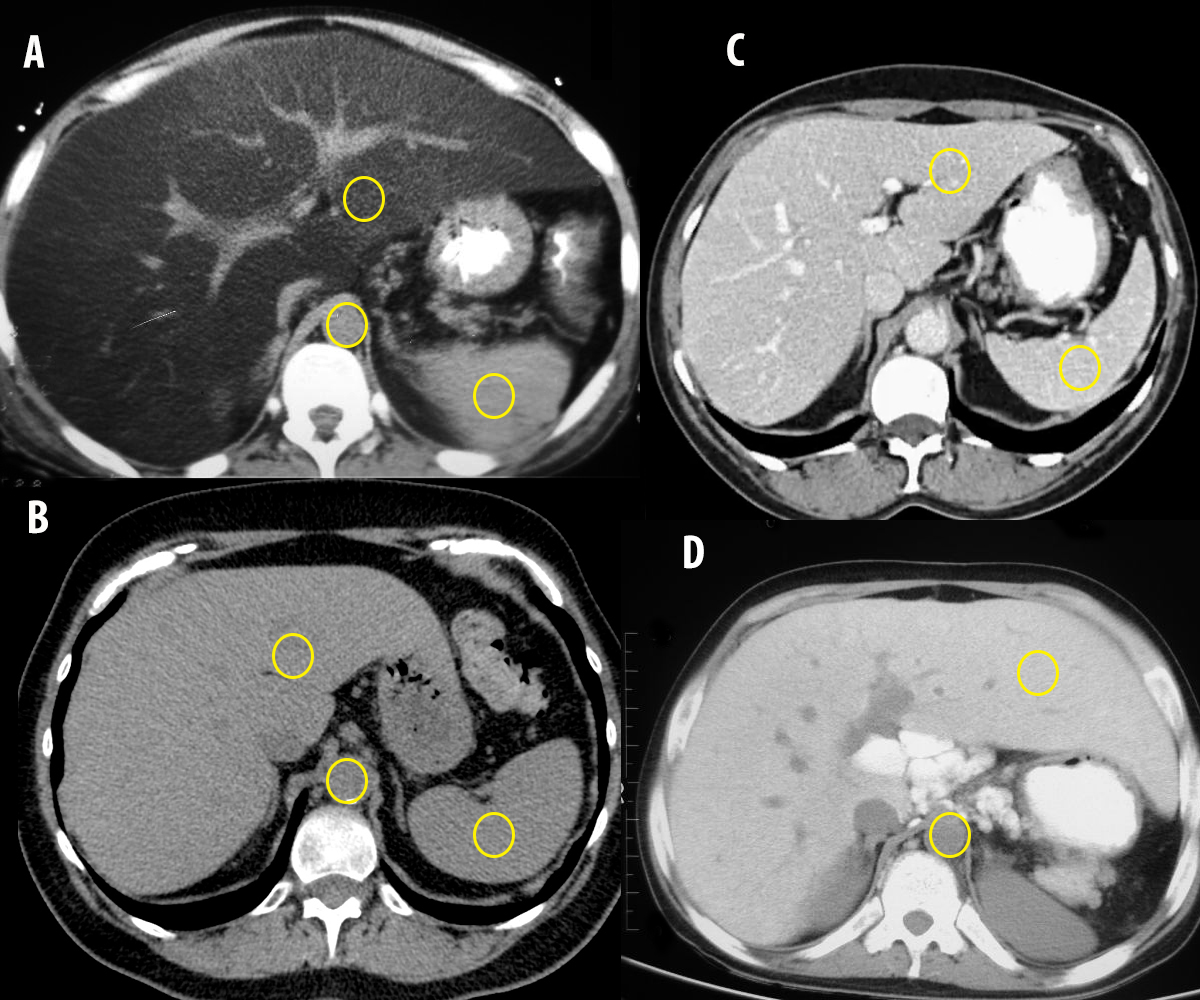
a) Decide which patients have received IV contrast first, as this will affect the density of parenchymal organs (liver, spleen kidneys) as well as blood vessels.
Using the density of the aorta relative to the crura of the diaphragm, Images A, B and D have no IV contrast. Note that GI contrast is present in all studies but B. In patient C, who did receive IV contrast, the liver and spleen enhance (show increased density) to a similar degree.
b) For the patients with no IV contrast, how would you expect the density of the liver to compare to that of the spleen, and to that of blood?
From visual inspection, the density of the liver and spleen should be relatively similar. If you do precise measurements by defining a region of interest and calculating the average Hounsfield units within that region, the normal liver is actually slightly more dense than the spleen, but it is hard to appreciate that slight difference visually. Similarly, unopacified blood should look similar to both organs, although precise measurements show blood to be slightly less dense than either liver or spleen. In fact, the amount of red blood cells in the blood (calculated as the hematocrit) will determine the precise density measurement of blood on CT. Patients who are severely anemic can have noticeably low blood density on CT.
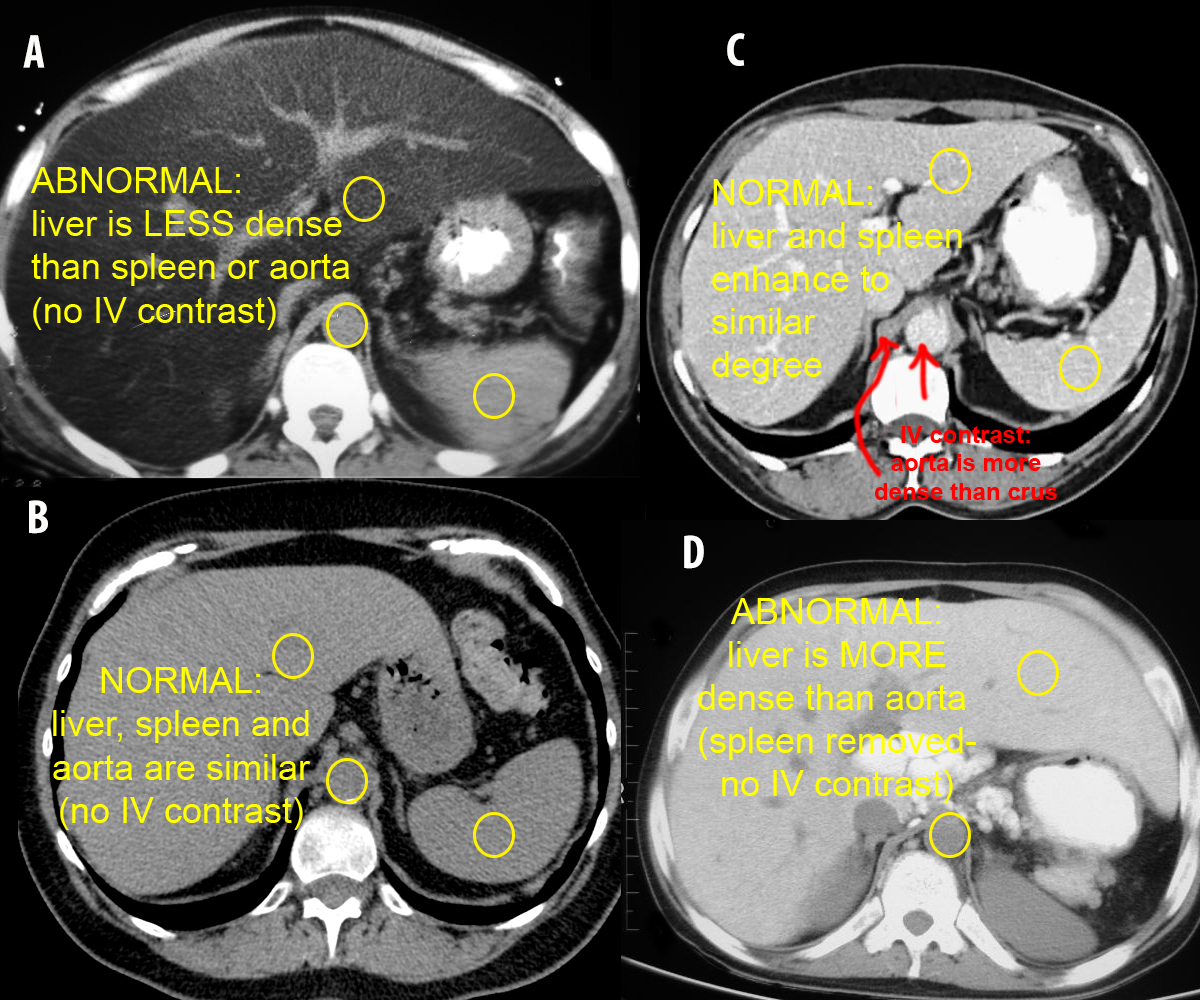
c) What do you think of the density of liver in patients A and D?
Patient B is normal (without IV contrast) so the density of liver, spleen and aorta all look similar. In patient A, the liver is noticeably LESS dense that aorta or spleen. This can be seen in fatty infiltration of the liver, which can occur in alcoholics or as a response to certain other toxins that damage the liver. In patient D, the liver is noticeably MORE dense than the aorta (this patient had their spleen removed, so it is not available for comparison). A very dense liver is often seen in patients who have received many blood transfusions due to iron buildup in the liver.
Abdomen Pelvis Case 1
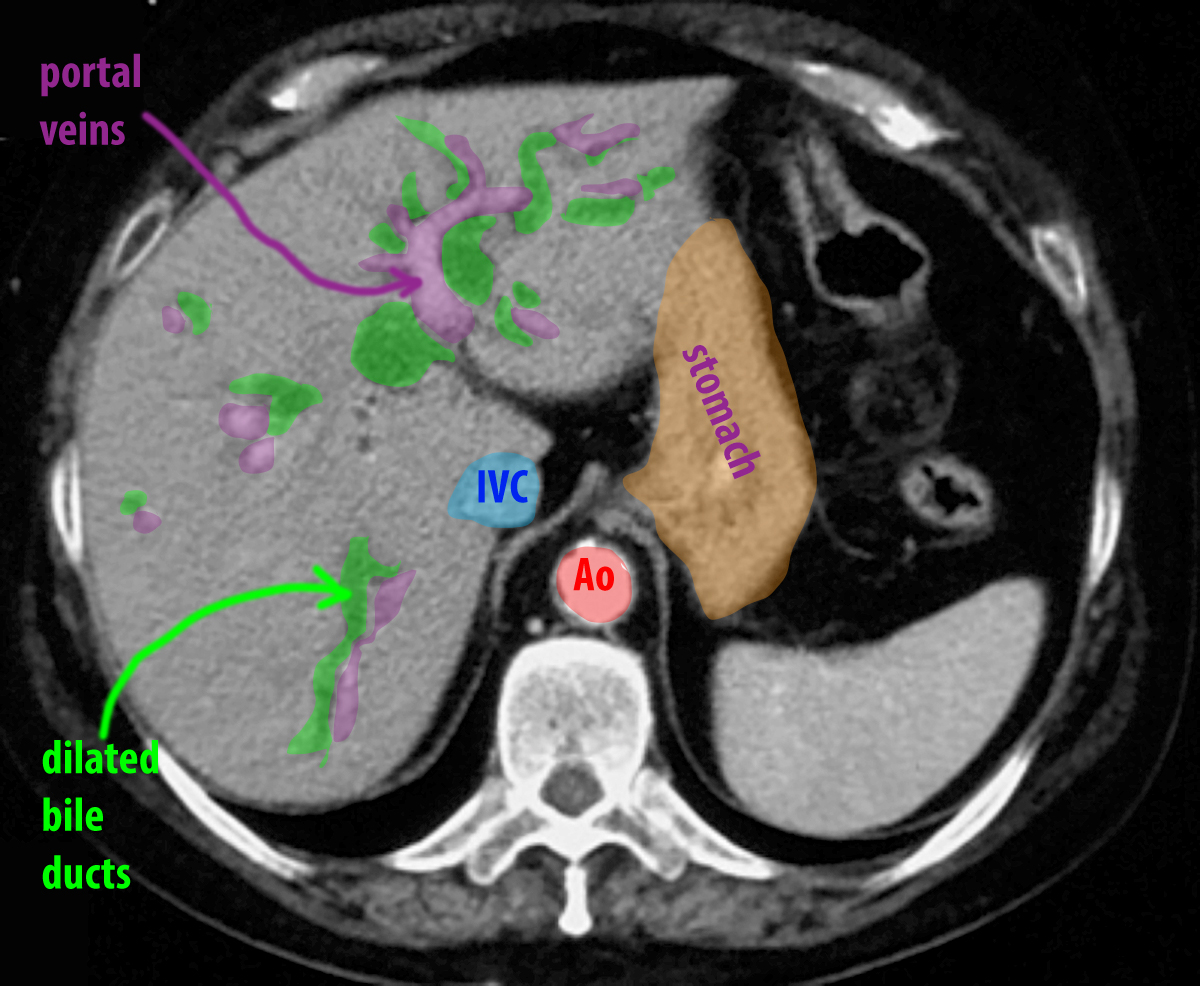
The liver is a complex organ, anatomically, with a dual blood supply and a tubular system for transporting bile to the GI tract. You are shown a CT image of a patient with chronic abdominal pain. Try to identify structures seen in the liver before clicking the labeled image.
Question 3:
a) What structures run with the bile ducts in the liver?
The bile ducts make up a part of the 'portal triad' within the liver, consisting of bile ducts, hepatic artery branches, and portal vein branches. So you will expect to see branching of all three of these systems together throughout the liver, at least on histologic images. Not all of these structures are normally large enough to see on CT scans.
b) What vessels in the liver are NOT part of the portal triad?
The hepatic veins drain blood from the liver into the IVC, and do not branch with the elements of the portal triad. You will see the largest and most obvious hepatic veins in the upper posterior part of the liver as they approach the IVC, while the largest portal veins will be seen in the lower and more anterior part of the liver.
c) Which vascular and biliary structures are normally visible in the liver on CT and which are not?
The hepatic artery system is hard to see on CT as the branches within the liver are quite small. They are generally only visible if scanning is done fairly early, when the contrast first reaches the upper abdominal aorta (where the celiac trunk originates). A few seconds later, they are no longer bright enough to be clearly seen. The portal venous branches are much larger and provide the majority of blood volume to the liver. They can be seen well on most contrast enhanced studies. The normal intrahepatic biliary ducts are too small to be seen on CT. The unopacitied hepatic veins can be seen early after IV contrast in the upper liver since they will be lower in density than surrounding parenchyma because the contrast has not yet reached them. On later scans, they enhance to a similar degree to the portal veins but are located superiorly in the liver and converging posteriorly toward the IVC.

Abdomen Pelvis Case 1
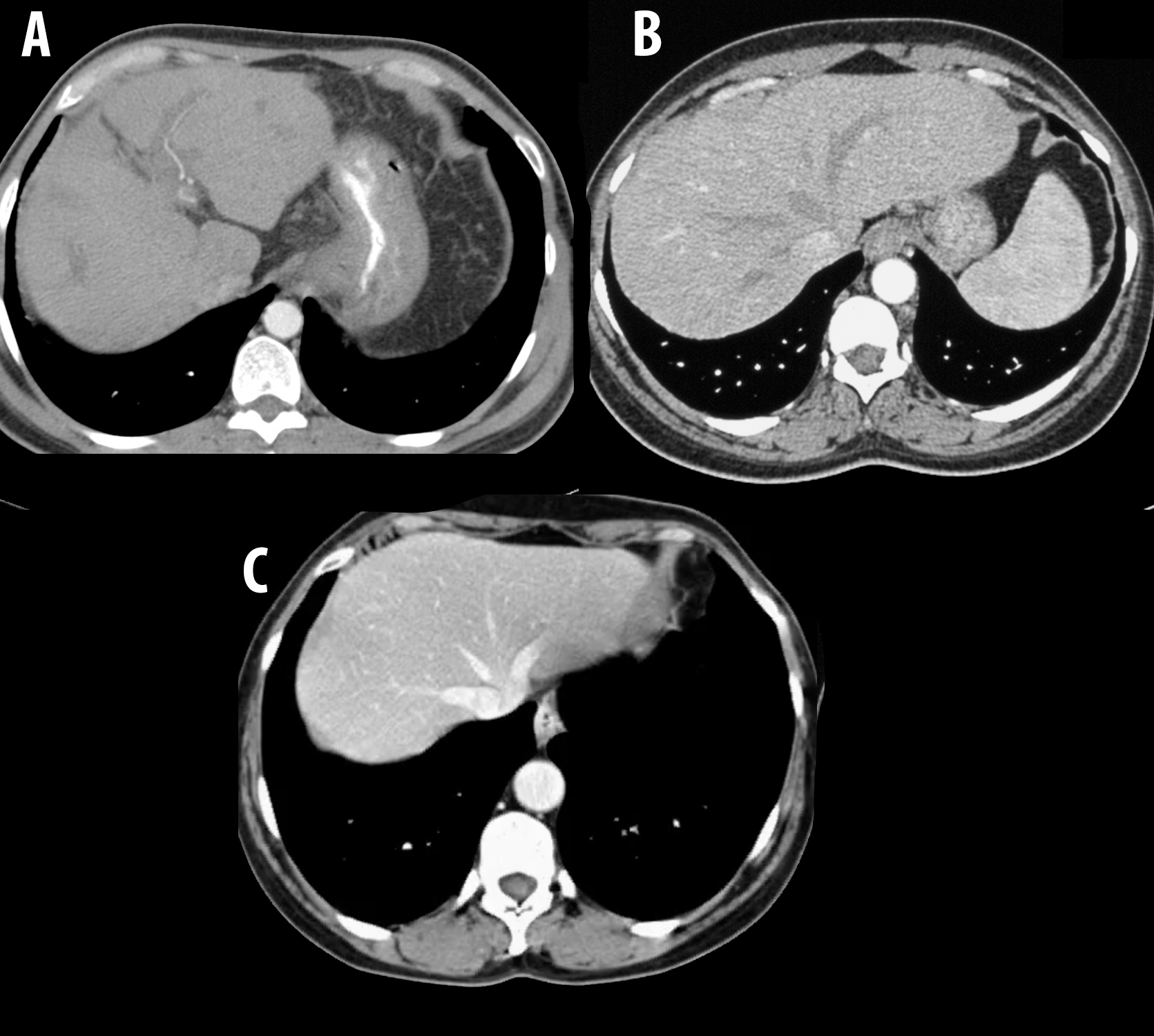
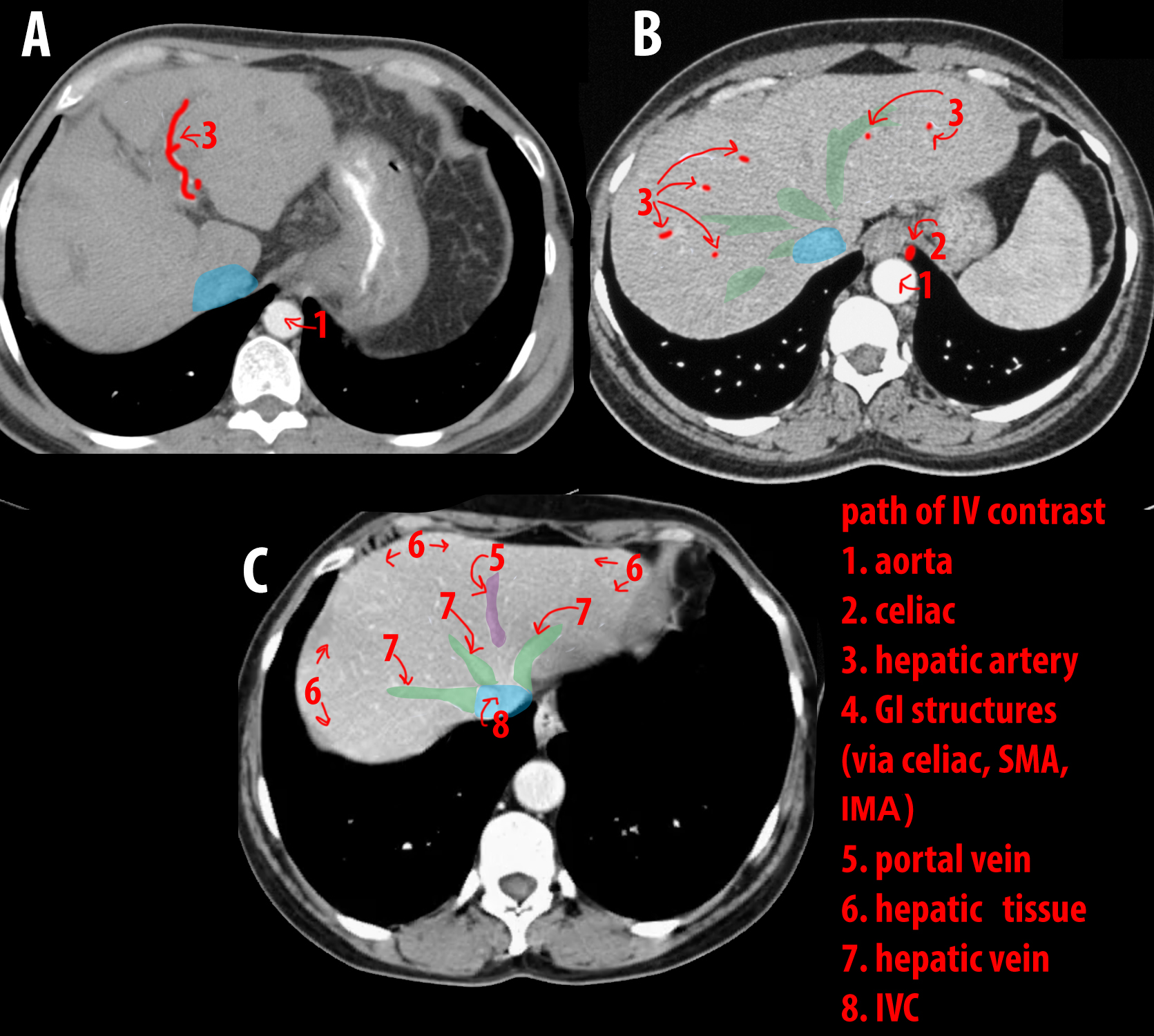
You are presented three images of the upper portion of the liver on axial CT, soft tissue windows. All have received IV contrast, but the three scans were obtained at different time delays after contrast administration. Image A is the earliest, Image B is slightly later, and Image C is the latest.
Question 4:
a) Examine the three studies and determine what vessels are visible in the liver on each. What enhancing vessel is seen within the liver on Image A?
Image A shows a single tiny bright vessel, which is consistent with a hepatic artery branch. These are only seen shortly after the IV contrast reaches the upper aorta and celiac trunk. They are too small to be easily seen on non-contrast images or on IV contrast images at later points in time.
b) How can you explain the difference in appearance of the vessels on Image B and Image C?
Image B is at a slightly later point in time than Image A, and is at a slightly higher portion of the liver. There are three vessels converging toward the IVC posteriorly, which appear less dense than liver parenchyma. These are the hepatic veins, which have not yet received contrast at this point in time. The liver tissue itself is slightly more dense than on Image A because the hepatic arteries and early flow from the portal system have made their way into the small vessels and capillaries of the liver tissue. On Image C, at a still later point in time, the contrast-laden blood from the capillaries in the liver has now reached the hepatic veins and made them (and the IVC) appear dense.