Abdomen Pelvis Case 4
82 year old patient with severe abdominal pain for the past few hours, now developing low blood pressure. Focus your attention on bowel loops in the pelvis.
Question 1:
a) What are imaging parameters for this study?
This is an axial CT displayed in soft tissue windows, with oral and IV contrast. The scan was obtained relatively early after contrast administration.
b) Where are the best places to look on a scan to determine timing of scanning after IV contrast?
There are several useful places to look, remembering that the contrast is given via an upper extremity vein. It will enter brachiocephalic veins, SVC, right atrium, right ventricle, pulmonary arteries, pulmonary veins, left atrium, left ventricle, and aorta before getting to any abdominal structures. So on an abdominal scan, comparing IVC to aorta is often helpful. Also the kidneys will display brighter contrast in the cortex than in the medullary pyramids early after IV contrast, and later on, the cortex and medulla will look similar in density. In the pelvis, you can compare contrast in the iliac arteries and veins, or in the femoral artery and vein, depending on the level you are looking at.
c) There are a lot of images in this series, so you are also given a select subset of images with a particular small intestinal loop highlighted on the images. What is abnormal about the course of this loop of bowel?
The small intestinal loop (highlighted in red) travels from abdomen into pelvis and then exits the pelvis to the medial left thigh, through the obturator foramen. This is an example of a type of hernia called an obturator hernia. These are not as common as inguinal hernias, but may be more concerning since the opening through which the bowel loop is traveling is very tiny. A herniation of a structure through a small, tight opening is hazardous because it may lead to compromise of blood flow to the herniated structure. In this case, the patient did require emergency surgery to resect part of her small bowel, which had lost its blood supply and had begun to deteriorate.
Abdomen Pelvis Case 4
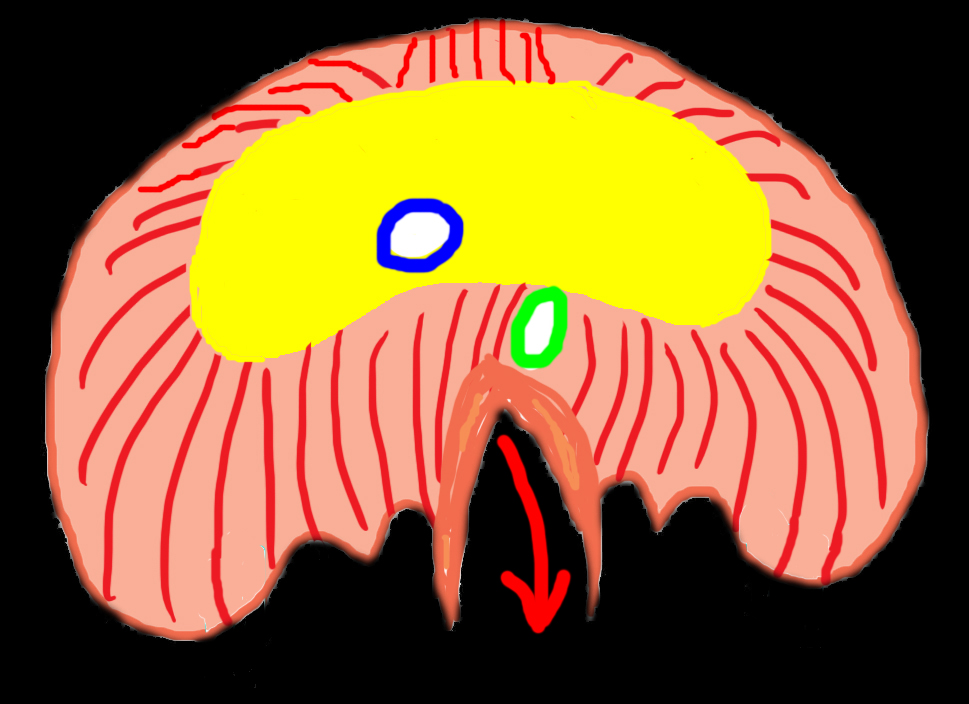
38 year old patient with heartburn. Focus your attention on the level of the diaphragm.
Question 2:
a) This is an axial CT without oral or intravenous contrast. What do you think of the appearance of the colon on the lowest slice?
The bottom image of the series shows some relatively dense material in the colon. While there is no oral contrast in the stomach or small intestine, this could indicate oral contrast given at an earlier time. Depending on how fast things are moving through the patient's GI tract (which varies widely from one patient to another), this contrast could have been given orally several days earlier.
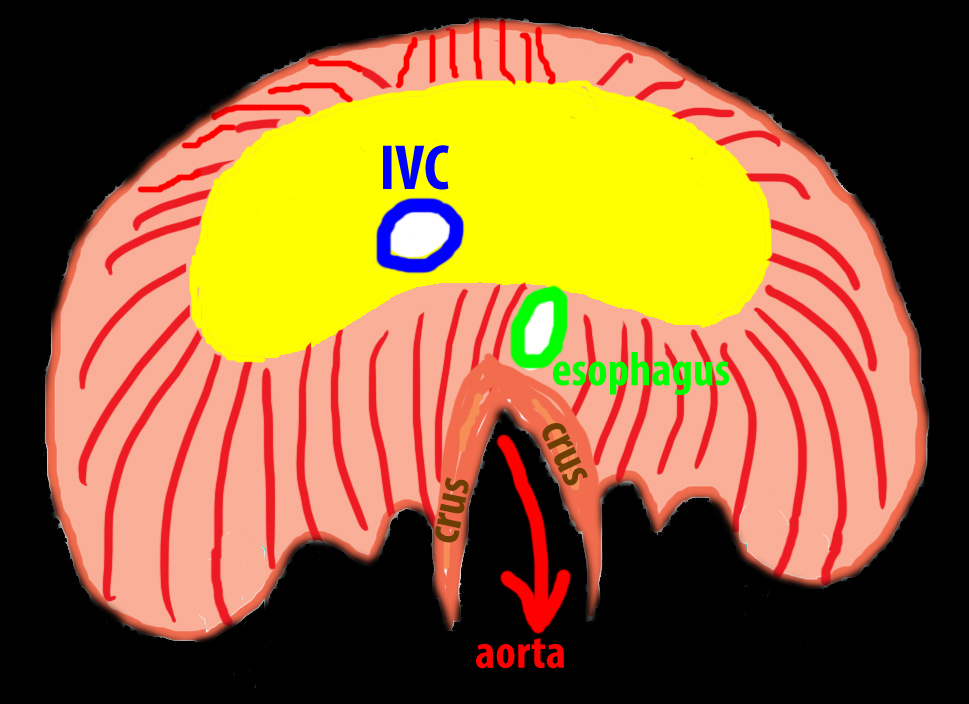
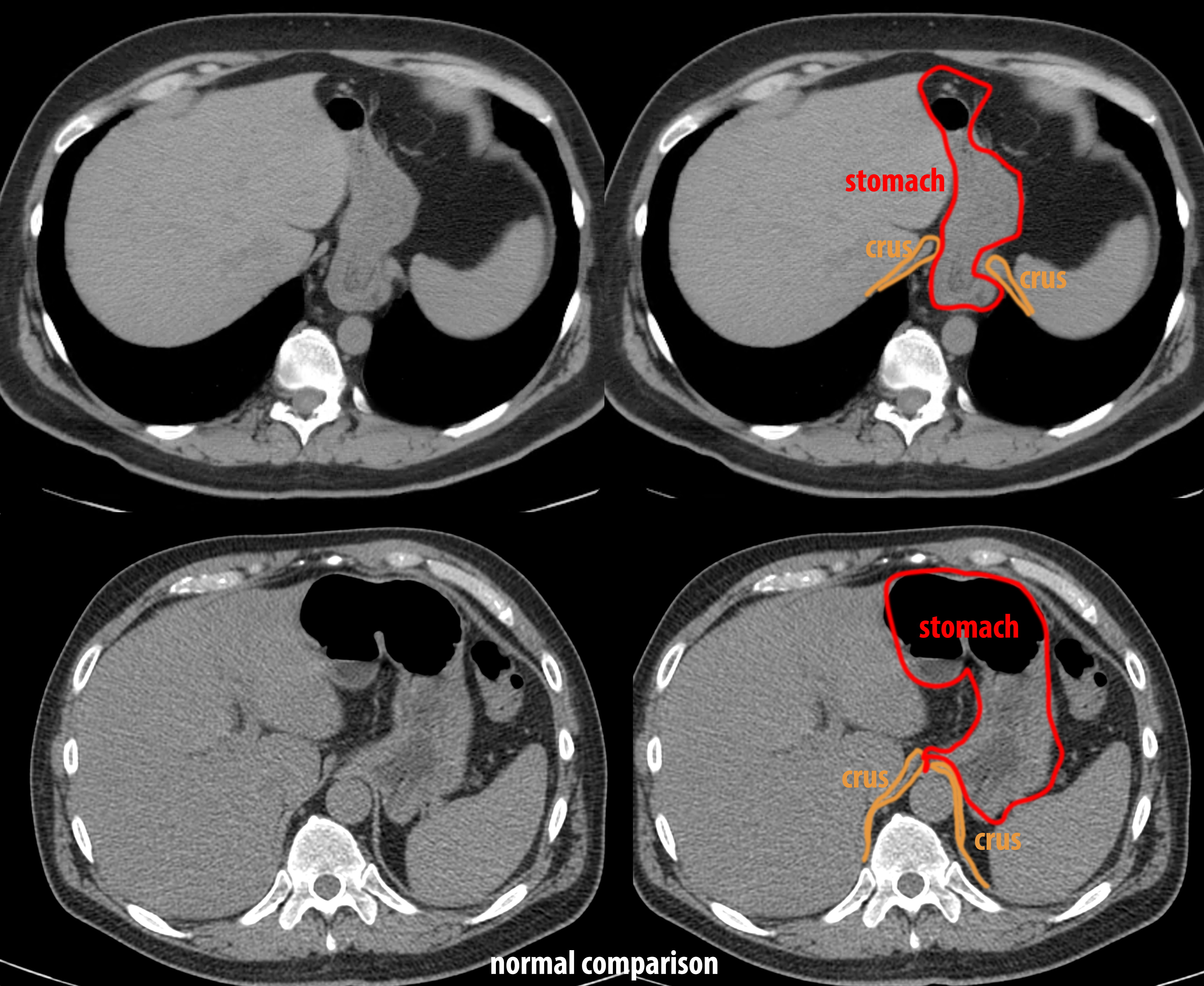
b) Focusing on the stomach, what do you notice about its position?
This is another example of a hernia, this time involving the stomach. The esophagus enters the abdomen through an opening in the diaphragm called the esophageal hiatus. So when the stomach comes back up through this opening, it is often called a 'hiatal hernia'. This is a small hiatal hernia, but even a small one can lead to symptoms due to reflux of gastric contents back into the esophagus. This is because normal function of the distal esophageal sphincter is partly enhanced by its placement within the muscular portion of the diaphragm. When the gastro-esophageal junction is not in its normal position, the sphincter may not longer be as effective.

Abdomen Pelvis Case 4
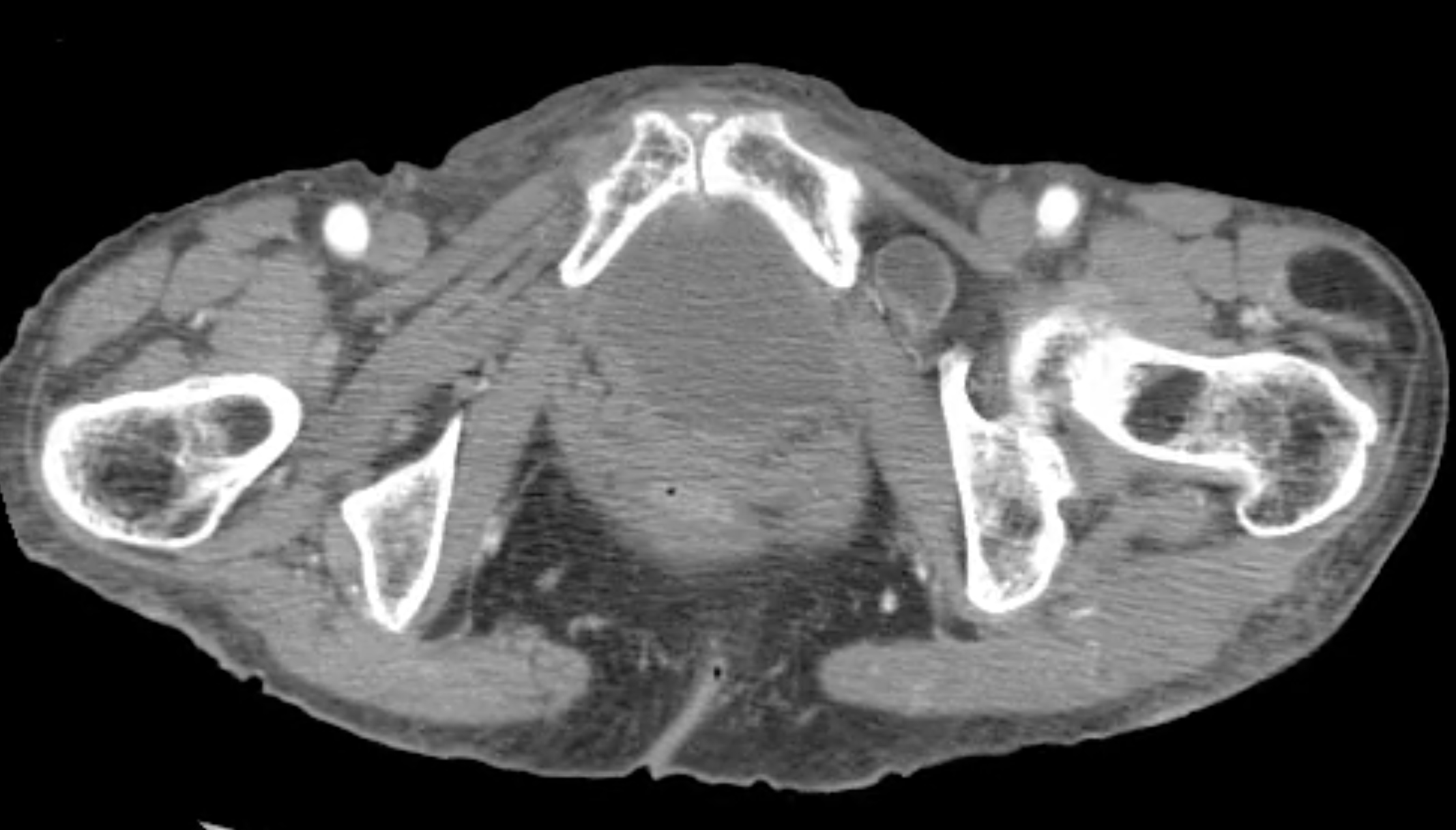
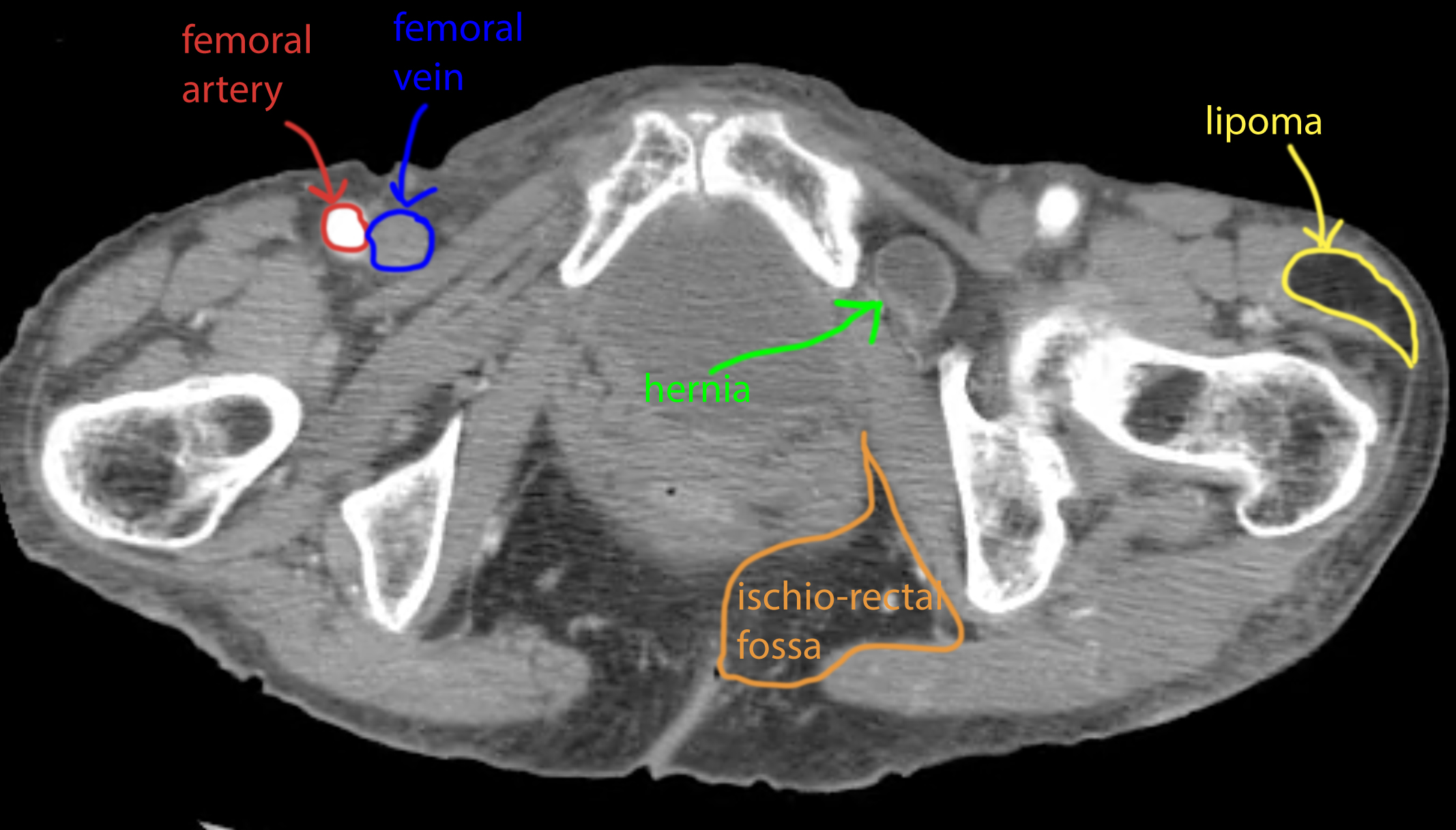
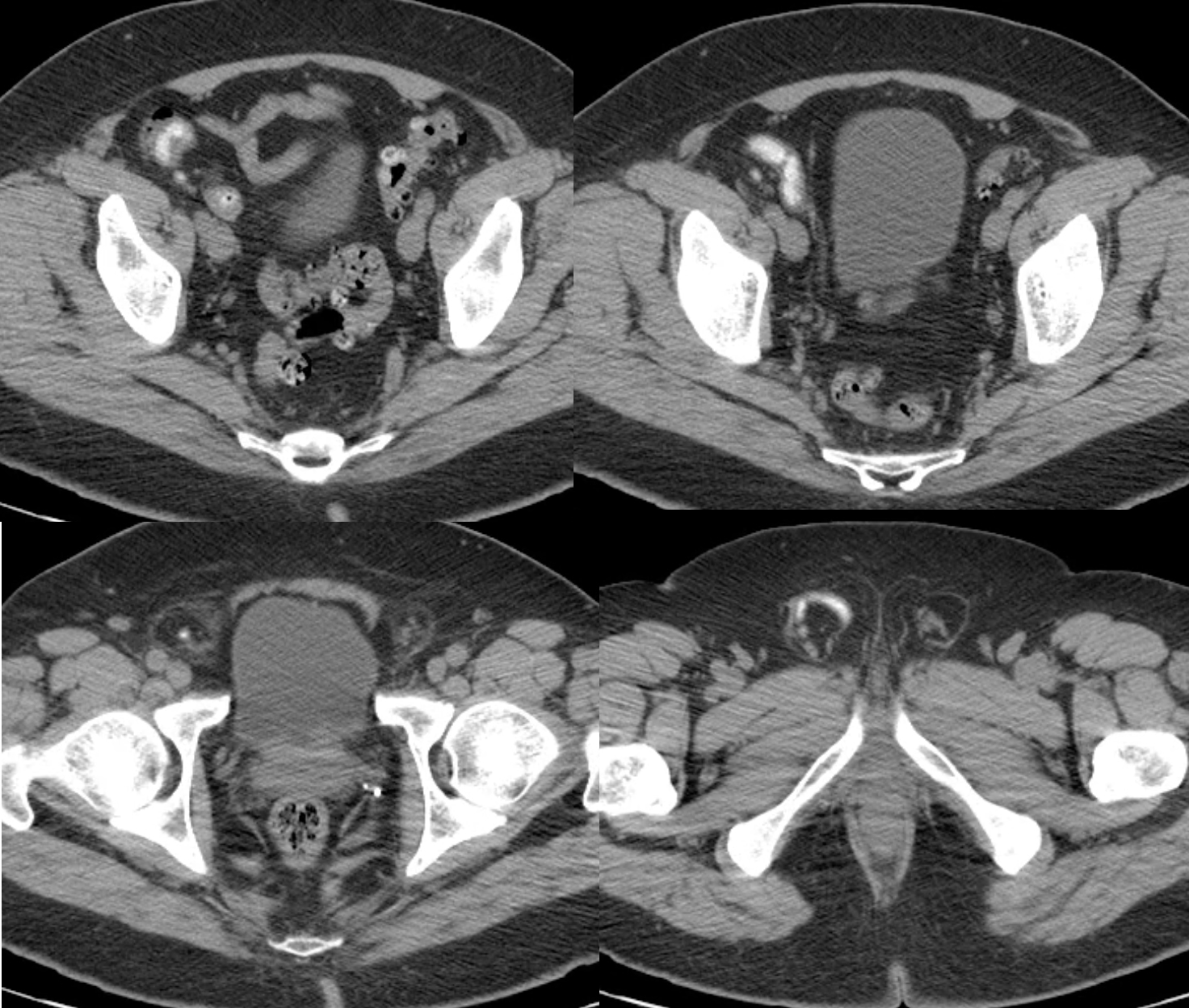
50 year old patient with vague right groin pain. As you look at the study, focus your attention on the right inguinal region.
Question 3:
a) Were IV or oral contrast given for this study?
Again, there are several loops of colon that seem to have small pockets of high density material in them. This might have been someone who had oral contrast given many hours to days in the past, with a small amount lingering in the colon.
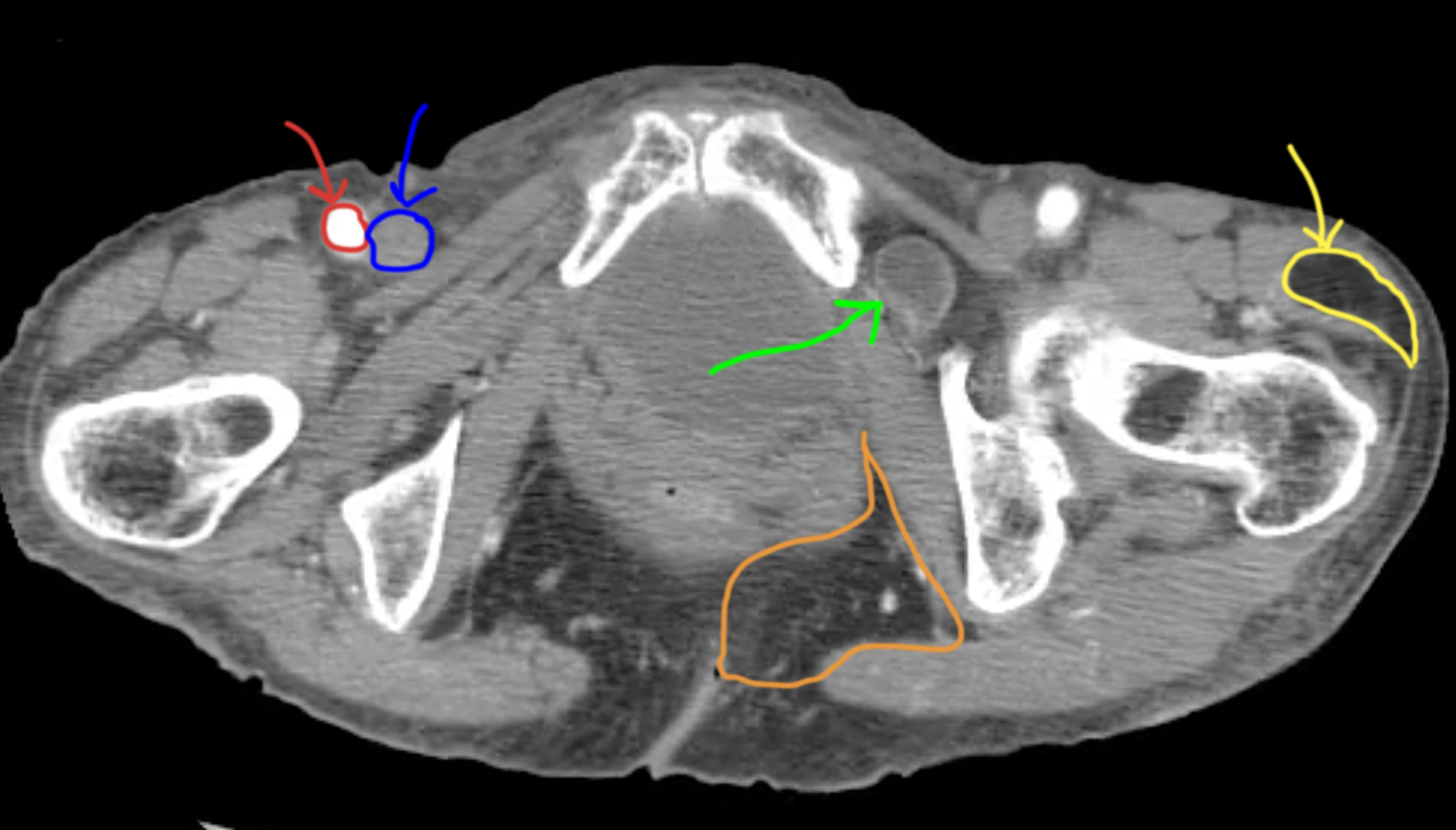
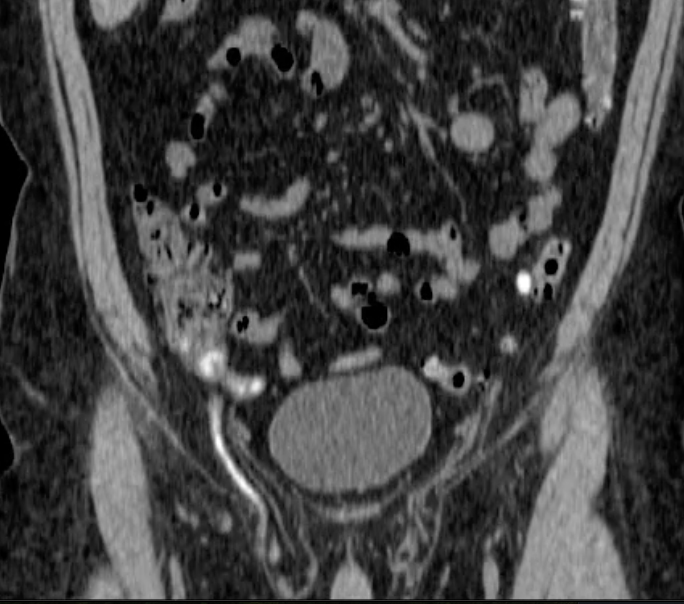
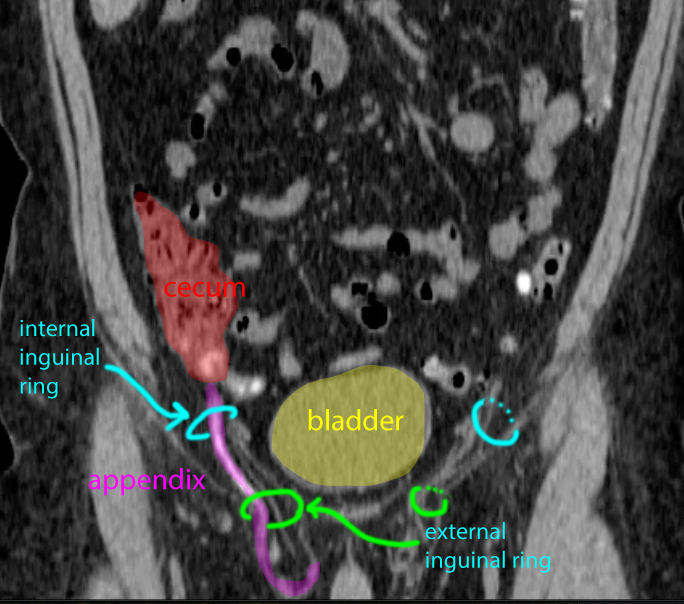
b) Why does the appendix appear high attenuation, and do you see signs of inflammation as would be present in appendicitis?
Oral contrast (or rectal contrast, which is sometimes given to evaluate specific problems in the distal GI tract) will often linger in parts of the colon. This patient has a few outpourings in their distal colon called diverticula, and much of the GI contrast is present in these rounded areas, which are prone to poor clearing of contents. This can result in inflammation in some patients, called diverticulitis. The appendix is a blind-ended tube and when contrast gets into it, the contrast often can also be seen for extended periods of time, as in this case. There is no stranding of the fat surrounding the appendix or the patient's diverticula. As you learned in the preview cases, stranding of fat is generally present in cases of inflammation. So this patient does not have findings that suggest either appendicitis or diverticulitis.
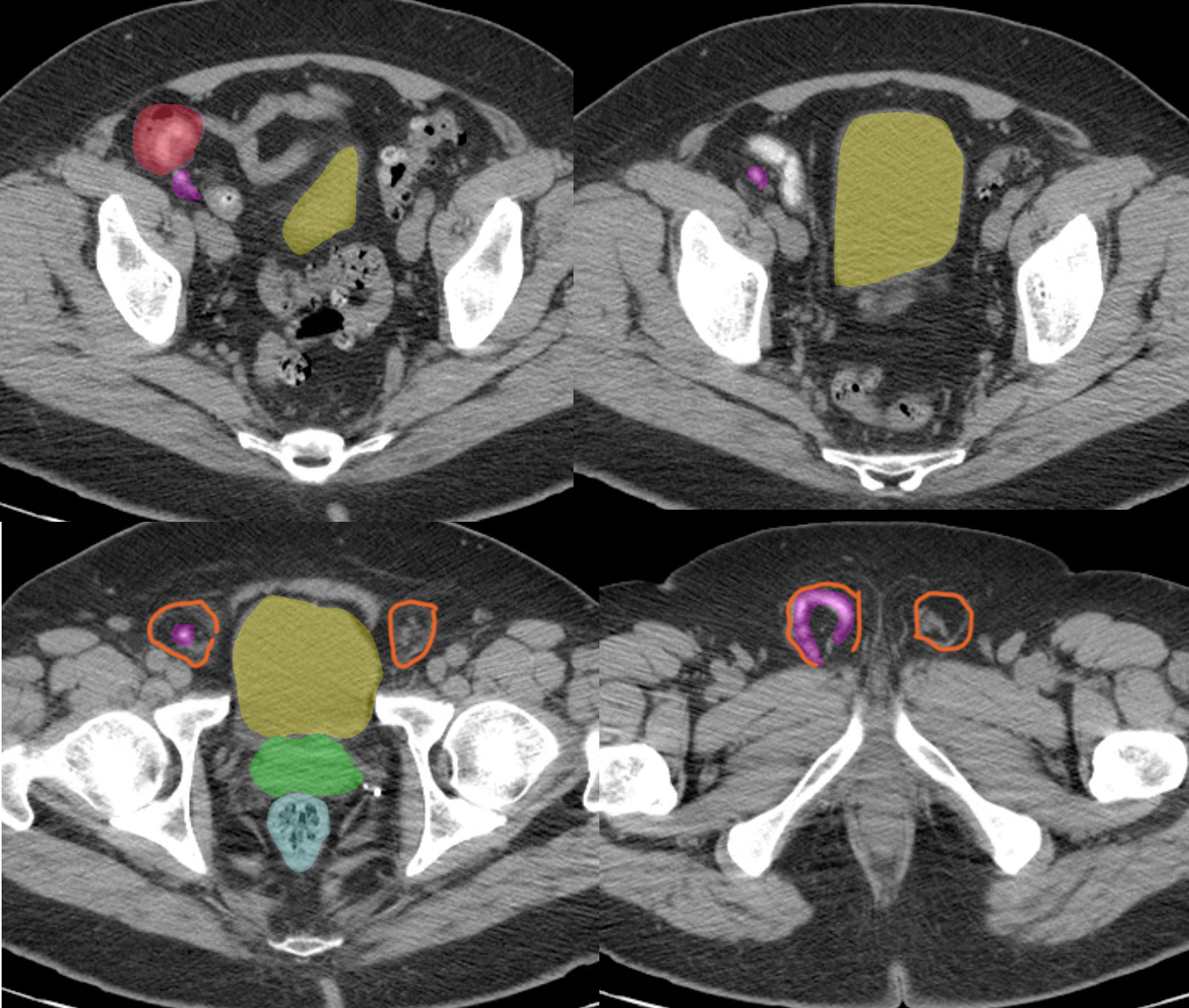
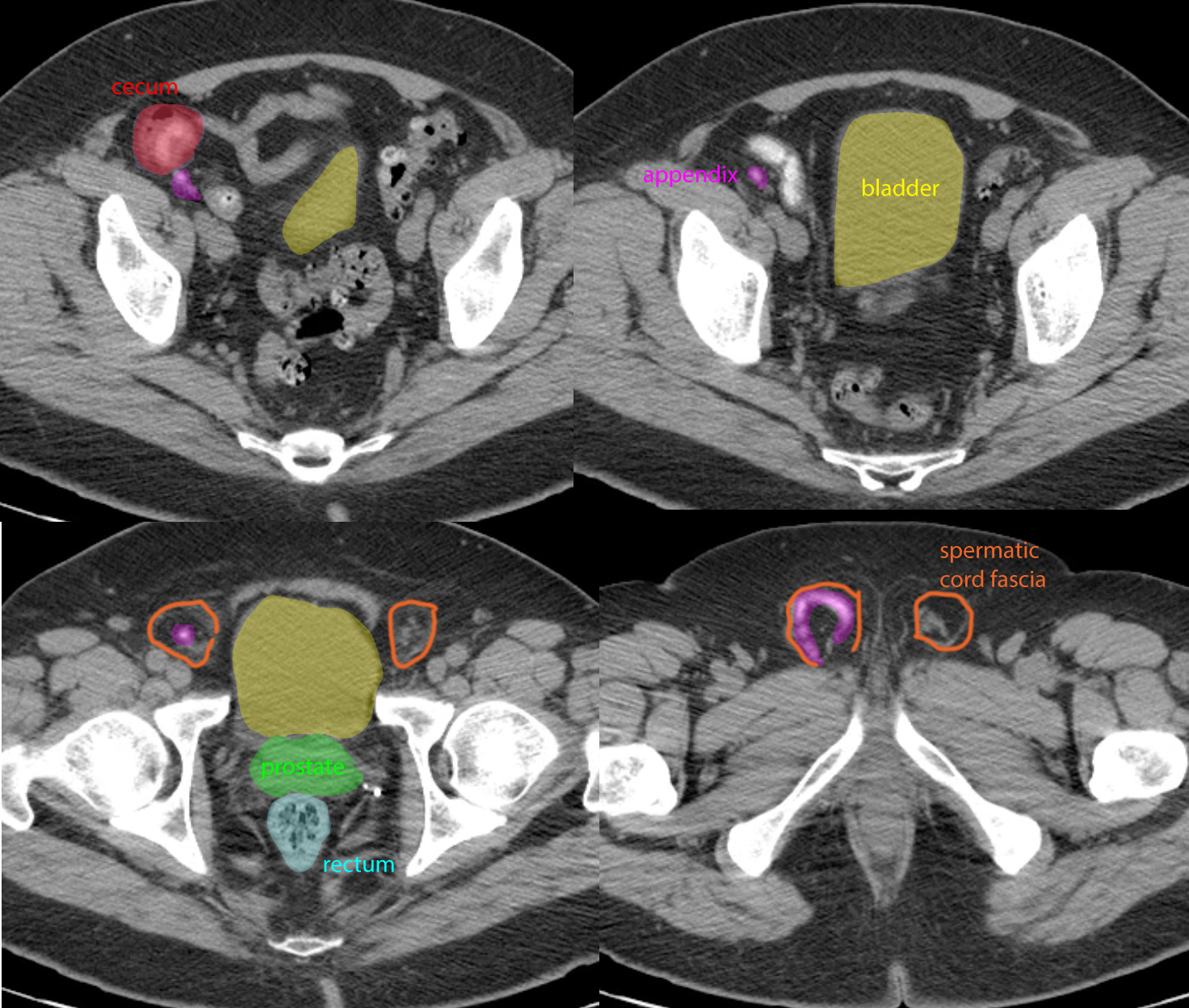
c) What unusual symptoms might this patient have if they later developed appendicitis?
Their pain would likely be localized in the groin and scrotum, given the location of their appendix, which has herniated into the inguinal region, through the inguinal canal, as shown in the labeled images below. This is a very unusual type of inguinal hernia. The more common inguinal hernia contains one or more loops of small bowel, or sometimes other pelvic organs such as sigmoid colon or bladder.
Abdomen Pelvis Case 4
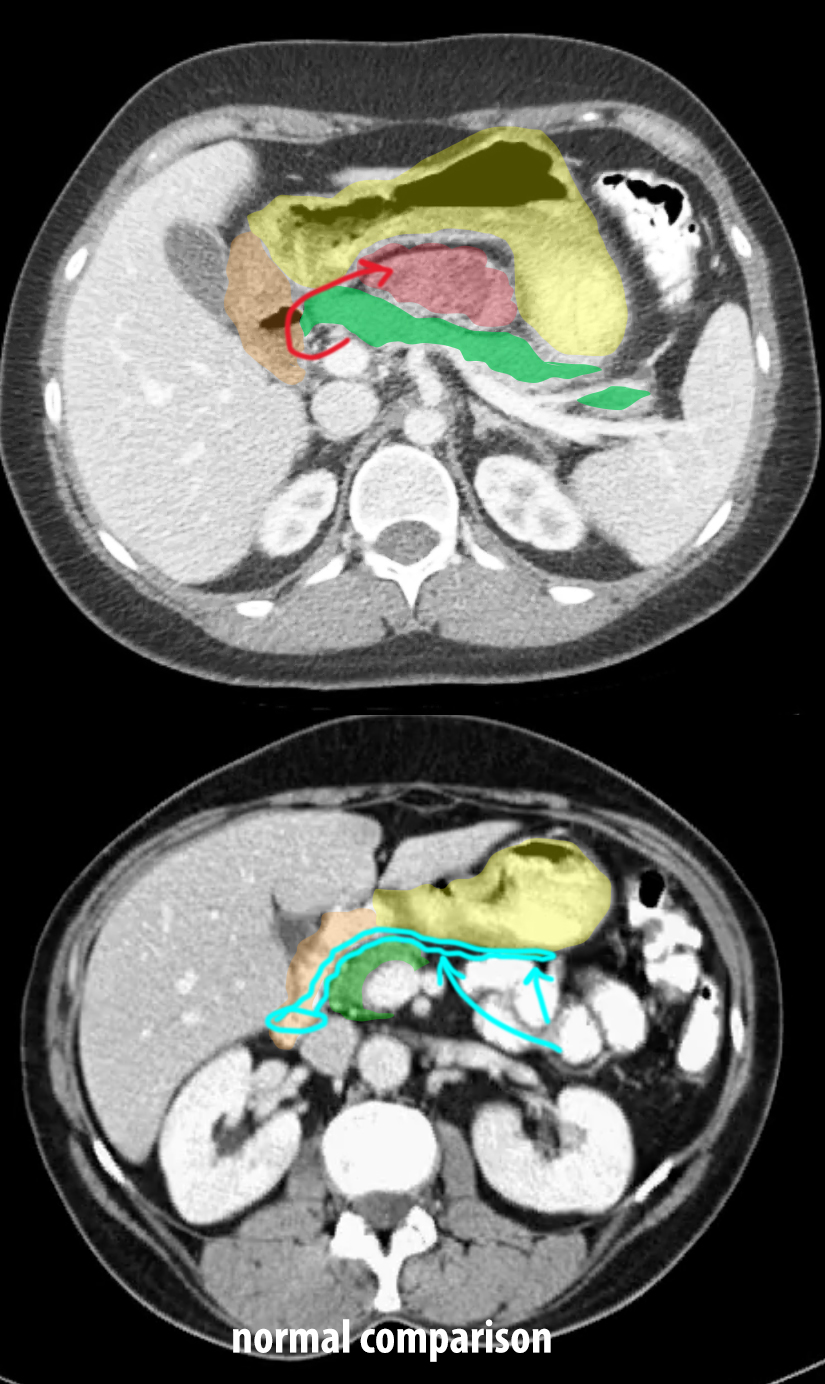
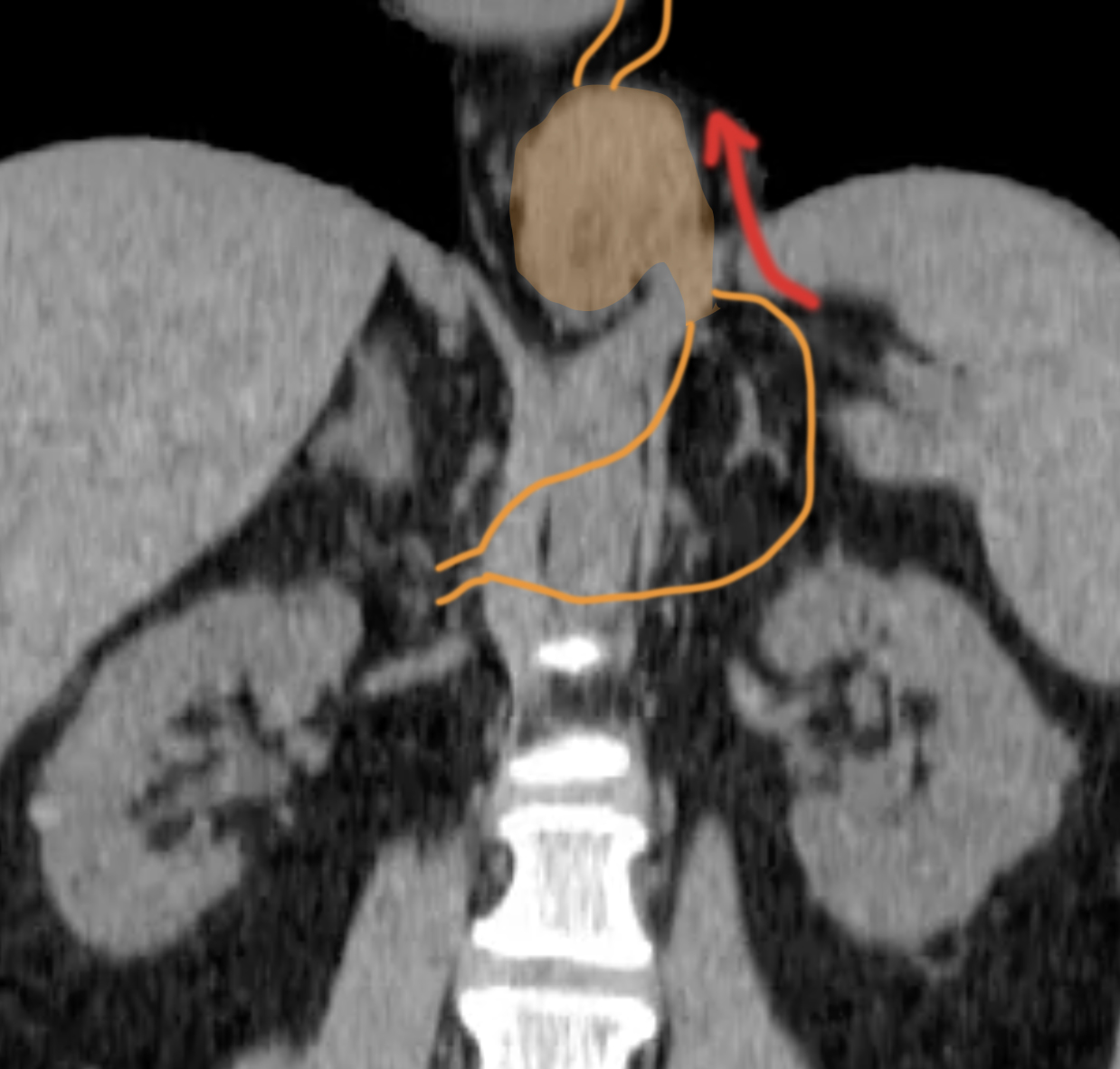
31 year old patient with left upper quadrant pain, intermittent in nature. Focus your attention on the lesser sac.
Question 4:
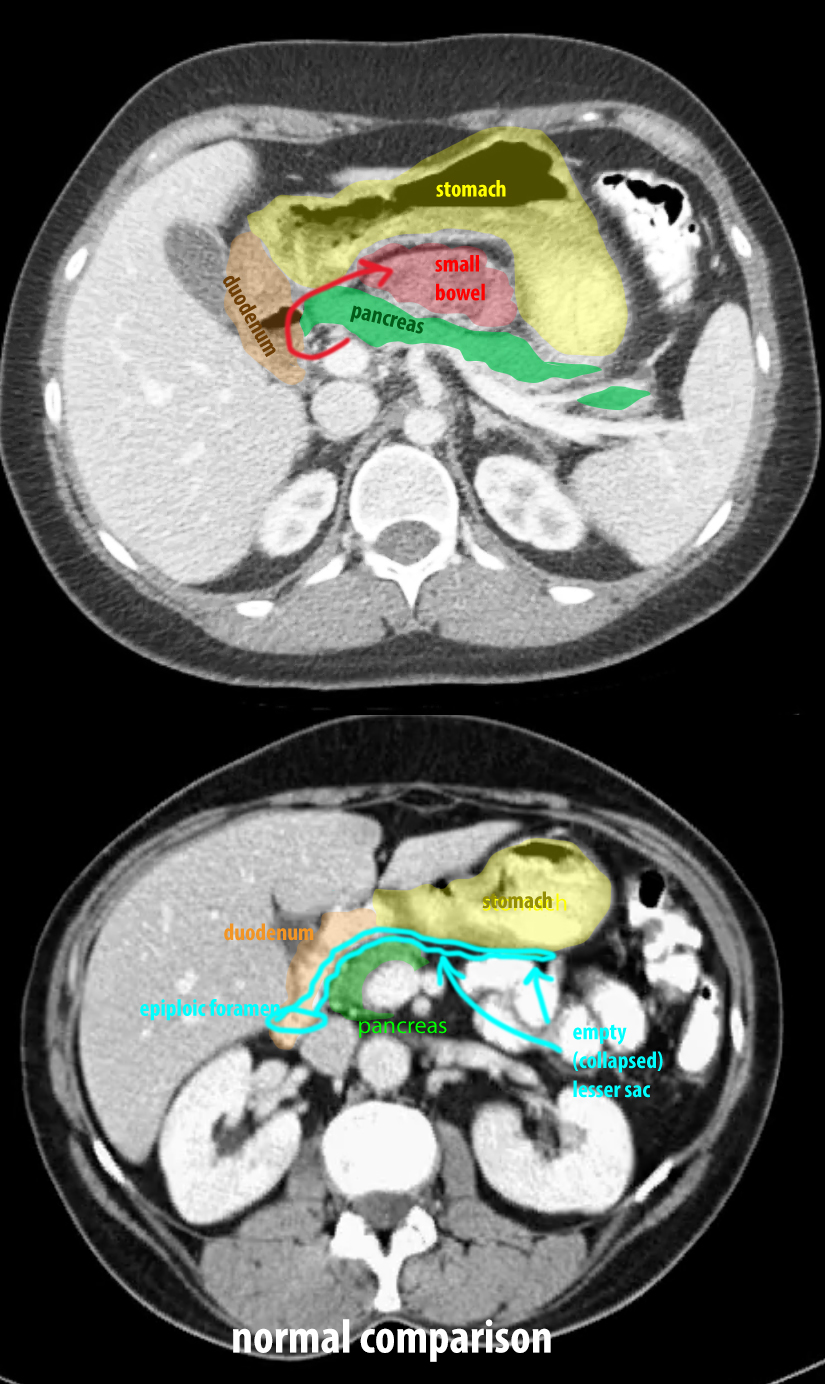
a) What organs are superficial and deep to the lesser sac?
The pancreas, duodenum and left kidney, covered by peritoneum, form the posterior boundary of the lesser sac. The posterior wall of the stomach, also covered by peritoneum, and the lesser omentum (gastrohepatic ligament) form the anterior boundary of the lesser sac. Normally, as shown in the labeled images below, there is nothing visible on CT between the posterior wall of the stomach and the pancreas, since the peritoneal layers and the small amount of normal fluid present are too thin to be seen. If you look on the labeled images below, you can see multiple bowel loops in the region that should not be there.
b) What is the definition of a hernia?
A hernia is a condition where a structure has moved from its normal position to another compartment of the body, through an opening in the compartmental wall. This can be a natural opening or a traumatic one (like from surgery or laceration). Often bowel is the thing that has moved through the opening, but other things can also herniate, such as fat, liver, spleen, bladder, etc, depending on where the opening is. We have seen examples of an obturator hernia (with bowel going through the obturator foramen), hiatal hernia (with stomach going through the esophageal hiatus of the diaphragm), inguinal hernia (with the appendix going through the inguinal canal), and now this example. This is called an 'internal hernia' because the opening is not in the body wall but deep in the abdomen. In this case, small bowel loops have herniated through the epiploic foramen, moving from the greater sac into the lesser sac.