Abdomen Pelvis Case 3
Four cases will be shown that all share abnormalities of one organ system. This is a study done on a 40 year old patient with vague left upper quadrant abdominal pain.
Question 1:
a) What do you notice as you go through these axial CT images about how the study was done?
This study was done with both oral and IV contrast. The axial images go through the kidneys twice. This is done so that the kidney can be imaged in the early phase of contrast enhancement, as well as in a later phase. Because the kidney functions to filter things from the blood into the urine, it has a very complex blood flow pattern and looks very different in the early phases of contrast enhancement compared to later, as blood moves from capillaries of the glomeruli and convoluted tubules (in the renal cortex) to the vessels surrounding the loops of Henle and collecting ducts (in the renal medulla).
b) What effect would this scanning protocol have on the patient radiation dose for the study?
Scanning at two different points in time would double the patient radiation dose. Sometimes we scan at three or four points in time, so every time we re-scan a body area, we are increasing radiation dose, and this should always be kept in mind to be sure that the multiple scans are really indicated and will give us important information.
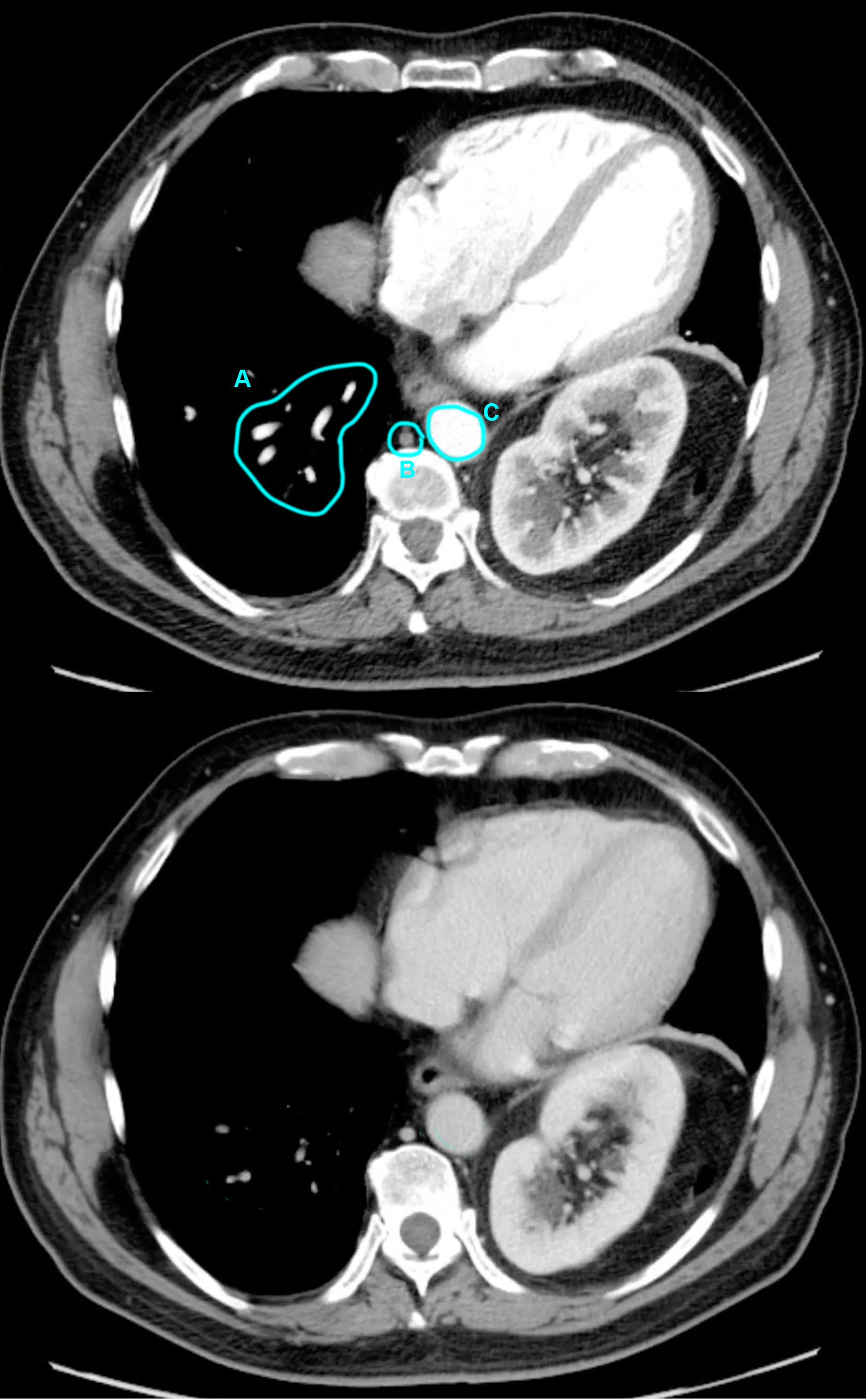
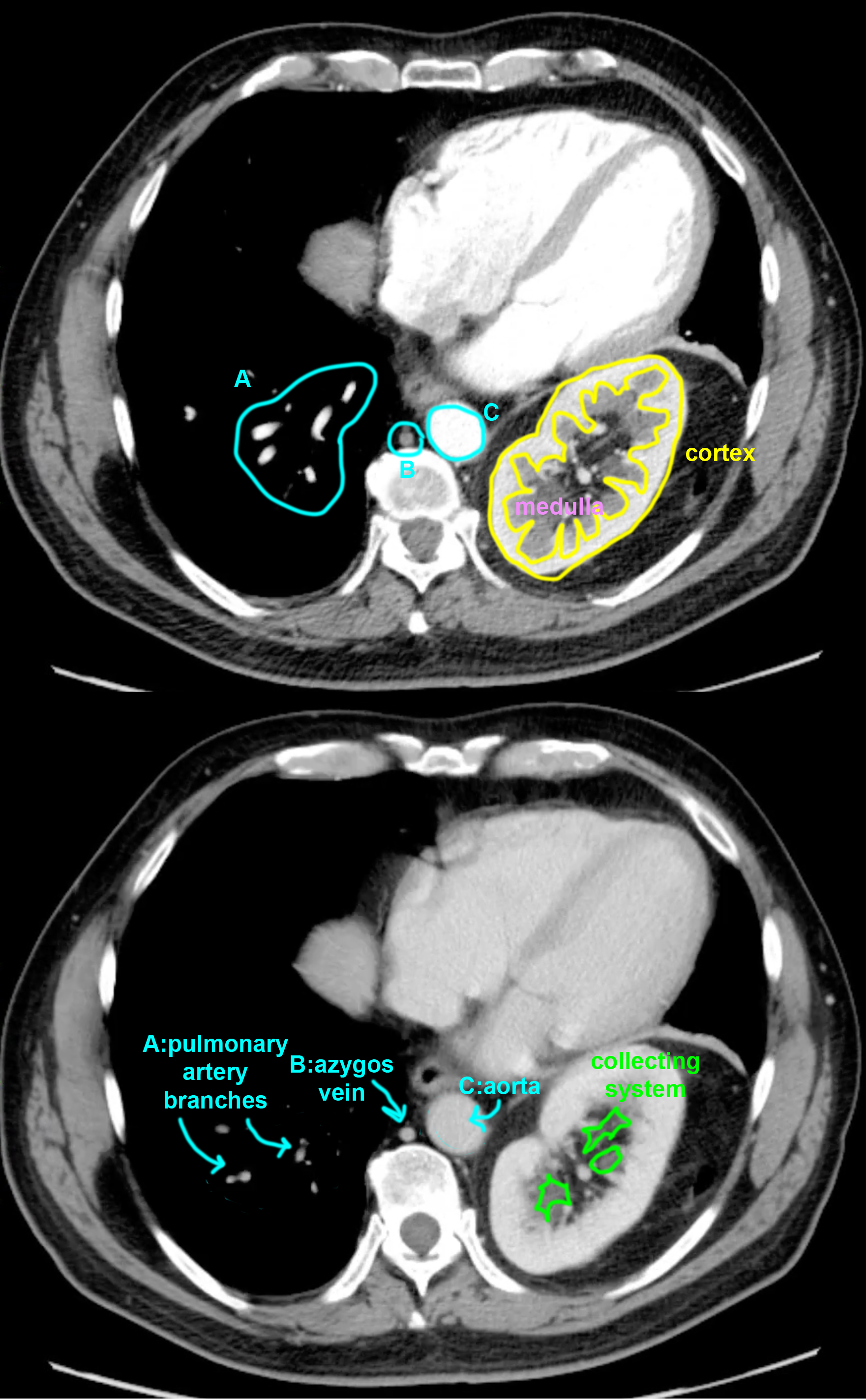
c) On the selected comparison images below, identify the labeled vessels and explain why their their density. as well as that of the kidney, differ on each image.
The answers are illustrated in the image below with labels. The contrast on the top image is brightest in the aorta (labeled C), as well as in the chambers of the heart because this image was obtained early after upper extremity venous injection. The vessels (labeled A) are also relatively bright and represent pulmonary artery branches. The cortex of the kidney enhances before the medulla on the top image. Contrast has not yet reached the trunk and lower body veins, like the azygos (labeled B). In the lower image, contrast has equilibrated in systemic arteries and veins, and all of the structures are similar in density, with loss of the differentiation between renal cortex and medulla.
Abdomen Pelvis Case 3
Another patient with abdominal pain and high blood pressure.
Question 2:
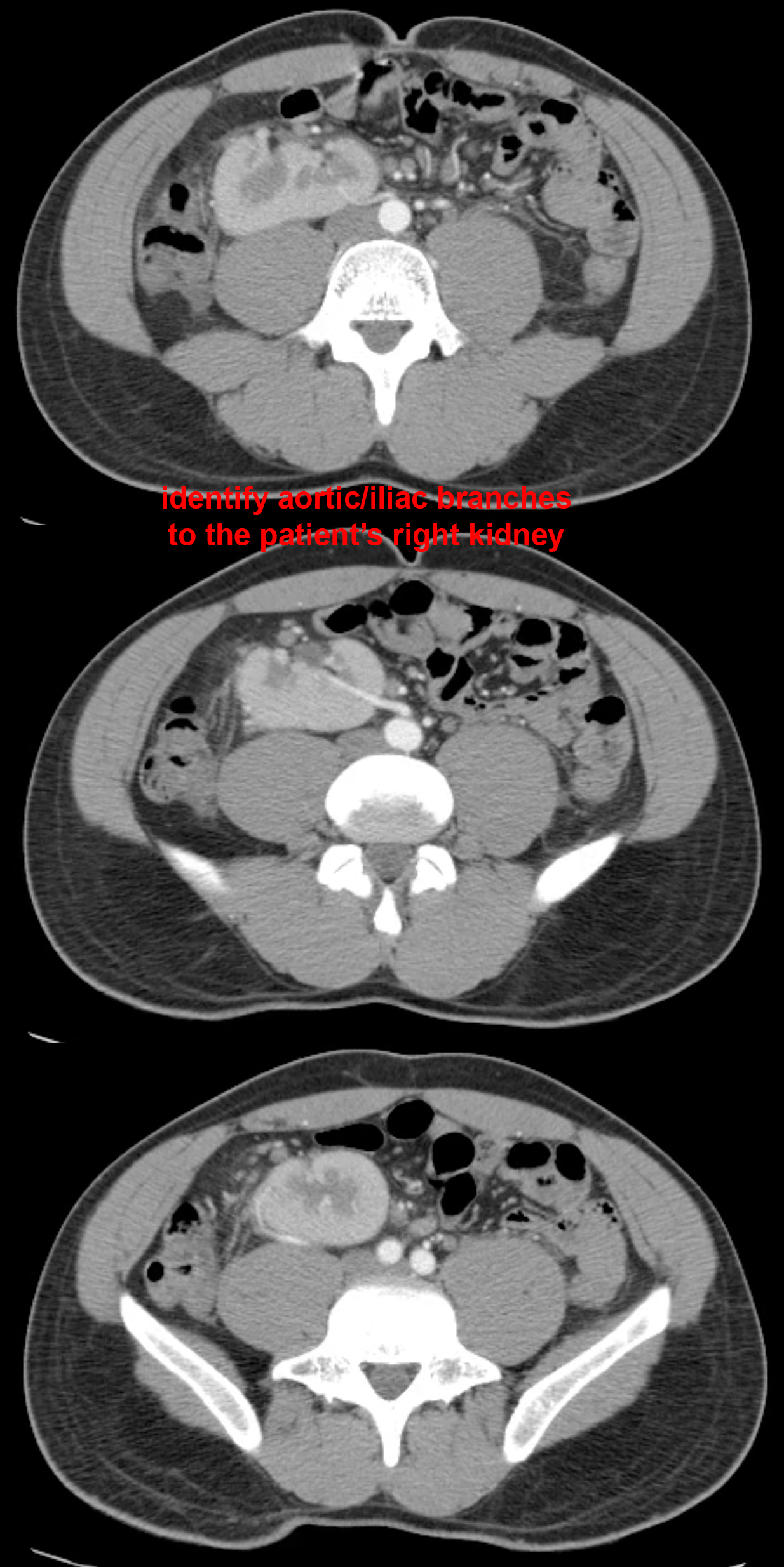
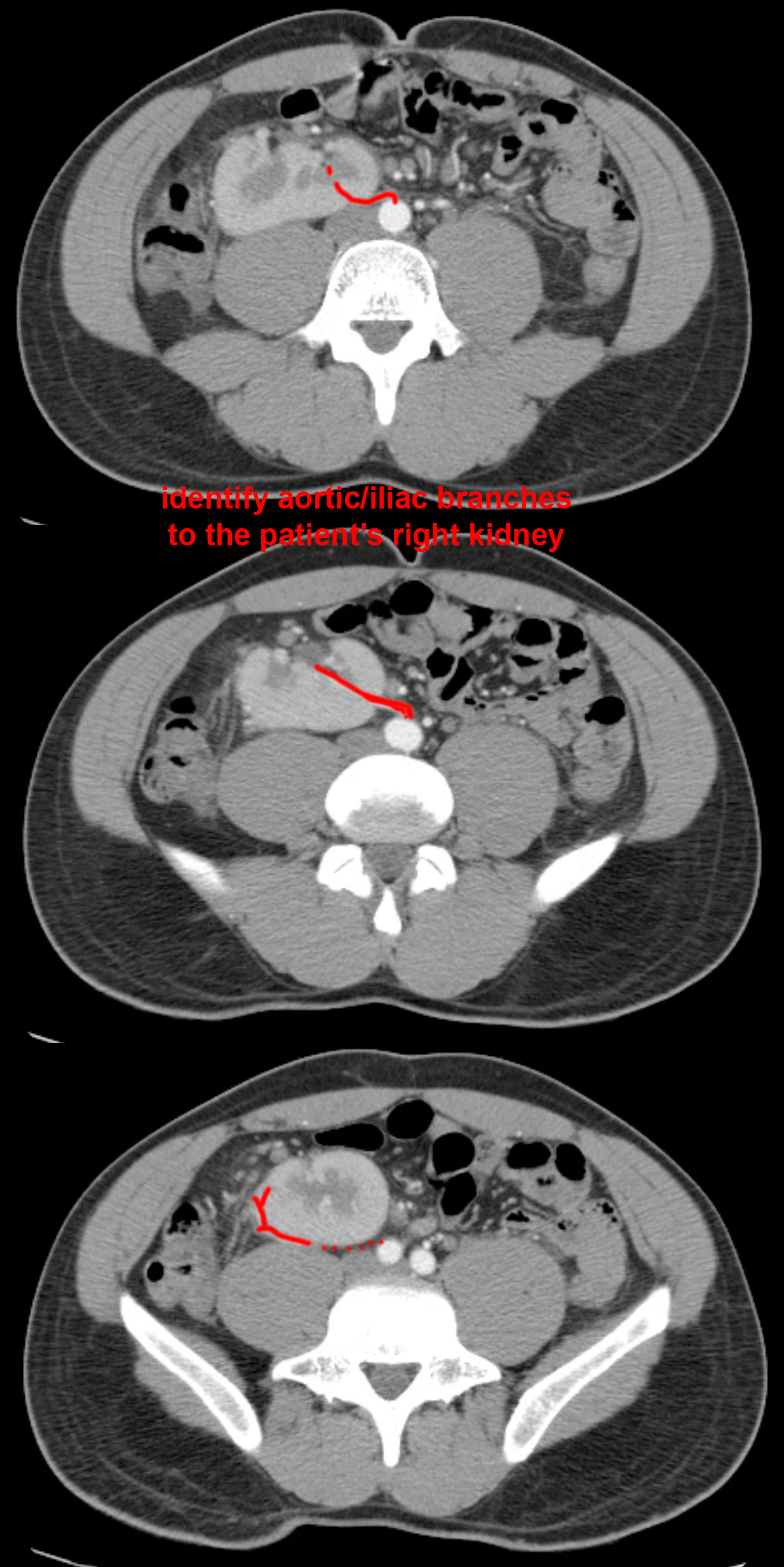
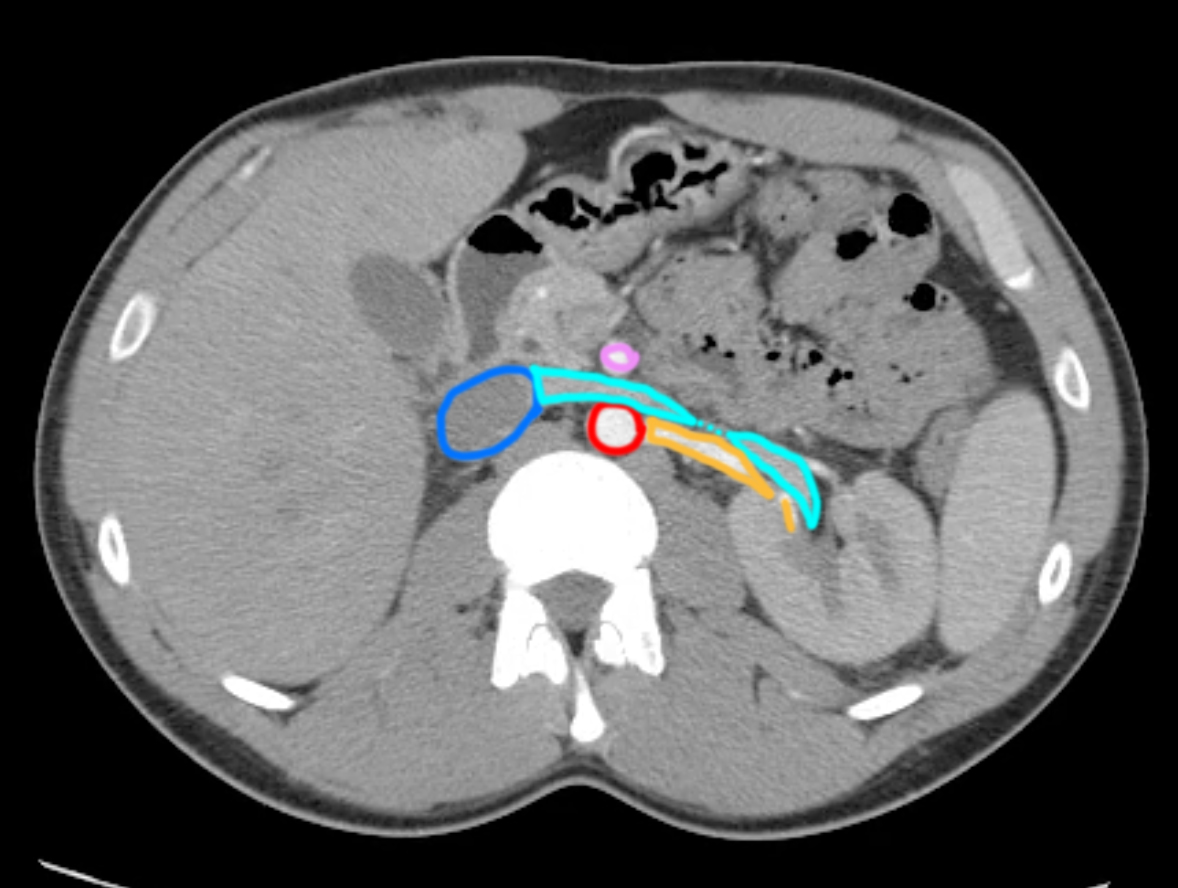
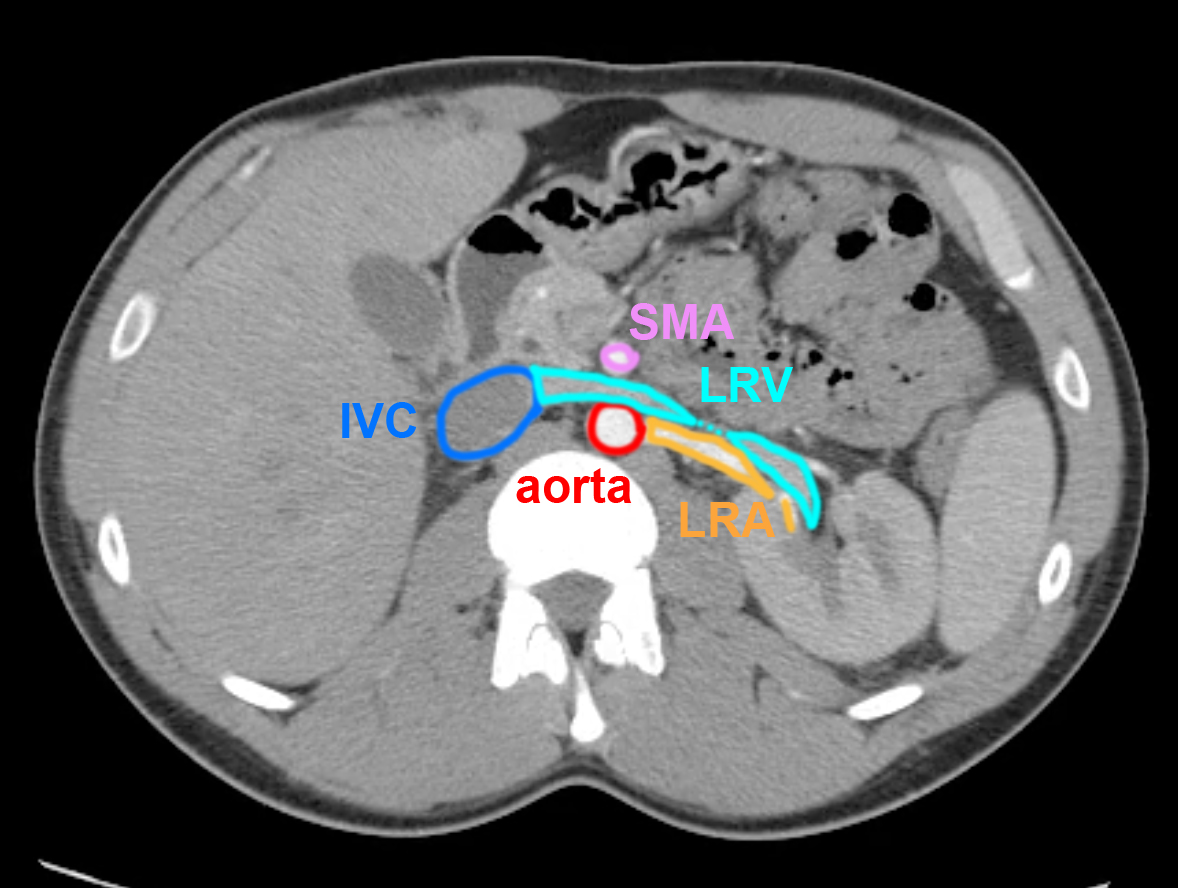
a) What do you think of the position of the right vs the left kidney in this patient? How can you relate this abnormality to the embryologic development of the kidney?
The right kidney is very low in position, located partly in the pelvis, and is also rotated from its normal orientation, with the collecting system emerging anteriorly rather than medially. The kidney and the gonad arise embryologically from the the same precursors, and the early fetal kidneys are both in the pelvis. They normally migrate upward until they reach the normal position, with renal arteries emerging form the aorta just below the level of the superior mesenteric artery (see normal renal artery image below). In this case, the migration on the right did not occur normally and the kidney remains in a low position.
b) What clinical effects might you expect from a kidney in this position?
Most pelvic kidneys are asymptomatic. Sometimes, if the course of the calyces and ureter are partly compressed, this may predispose patients to urinary tract infections. Also, since the kidney typically acquires blood supply from sequentially higher and higher aortic branches as it migrates, a pelvic kidney may have abnormal blood vessels that are in unusual courses, and this can lead to hypertension through disruption of the usual blood pressure control mechanisms which have to do with renal blood flow. Look at the selected images below to see what type of blood supply this abnormal right pelvic kidney has in this patient.

Abdomen Pelvis Case 3
This patient has chronic right flank pain and had hematuria ( blood in urine ) in the past but not now.
Question 3:
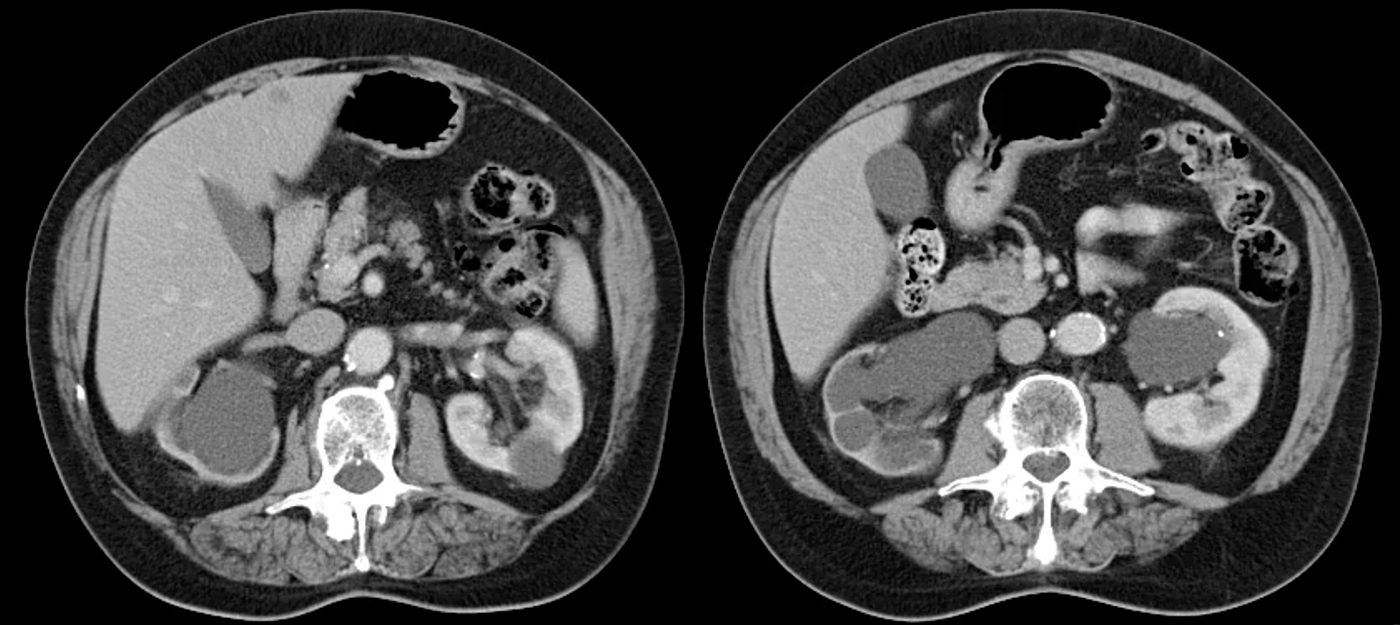
a) What do you think of the thickness of the kidney tissue on the patient's right vs the left?
The thickness of the right kidney parenchyma is much thinner than the tissue of the left kidney, which appears normal.
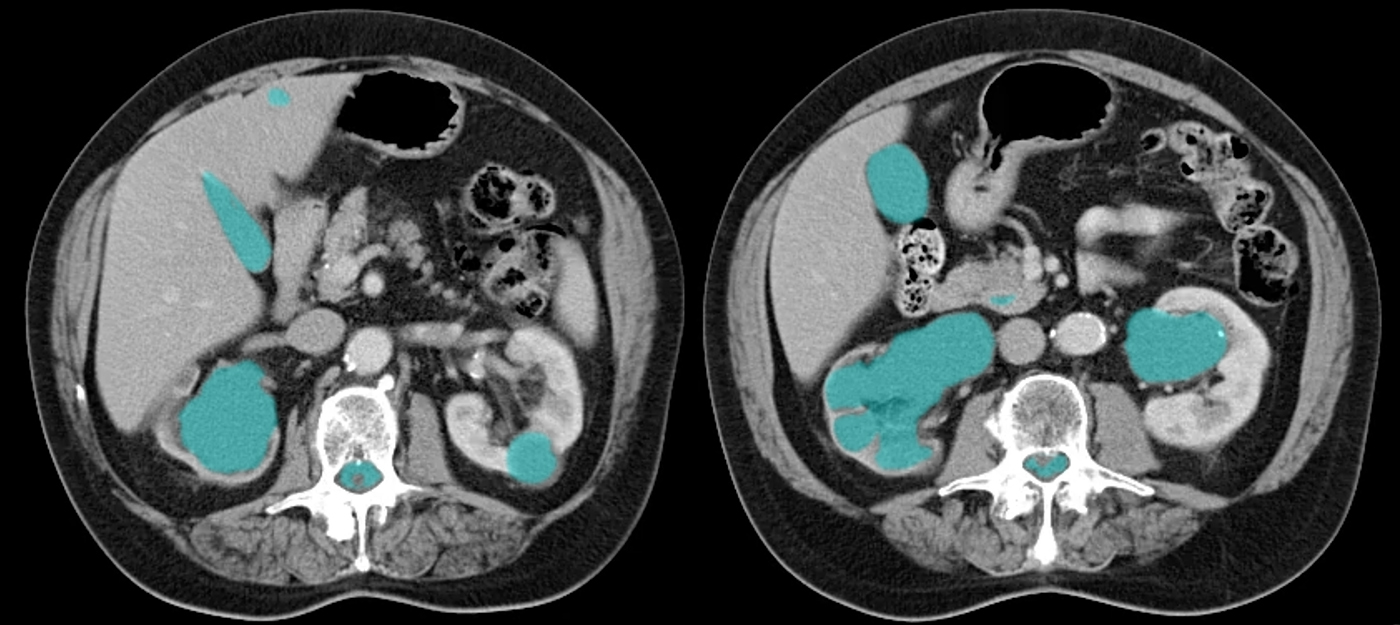
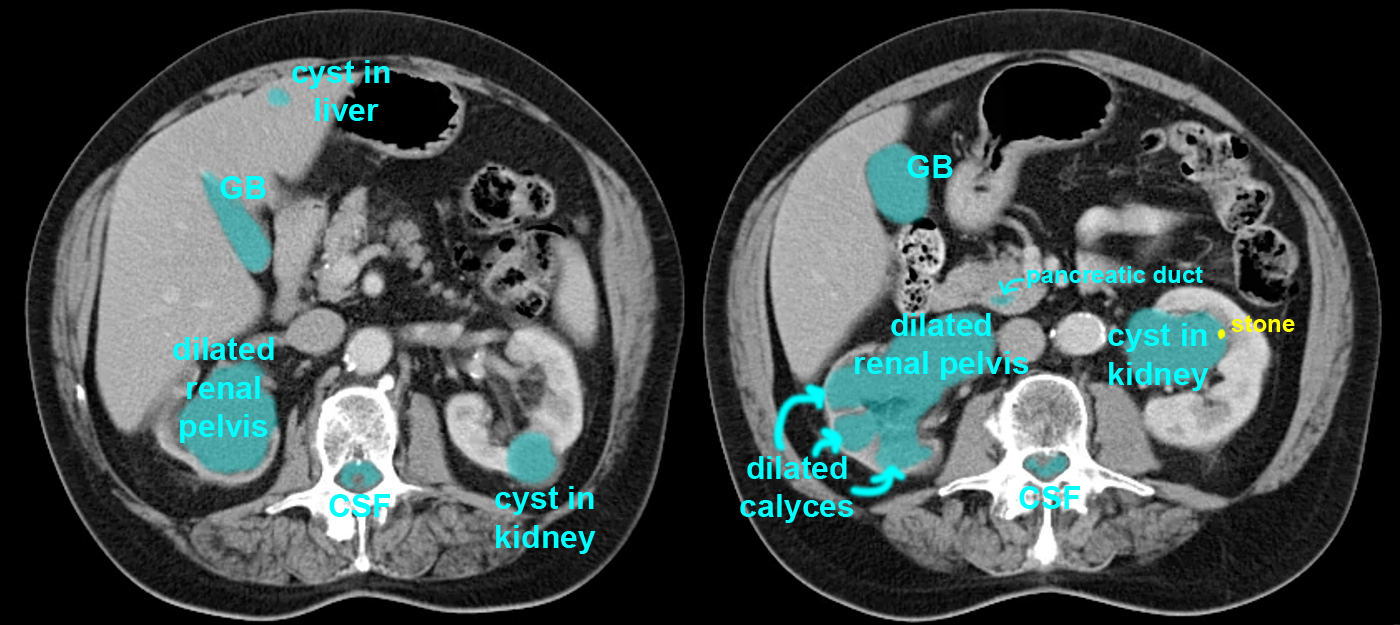
b) What do you think of the renal collecting system (calyces and renal pelvis) on the right vs the left?
There is a dilated fluid-filled structure located centrally on the right, which has a number of rounded protrusions into the thinned rim of renal tissue. This appearance is most consistent with a blockage of the urinary system, resulting in a ballooning out of the renal pelvis and calyces as seen here.
c) Is the left kidney normal?
There are small and larger rounded fluid-filled masses on the left, which are typical for benign renal cysts, a common finding in many patients and usually not associated with any problems for the patient.
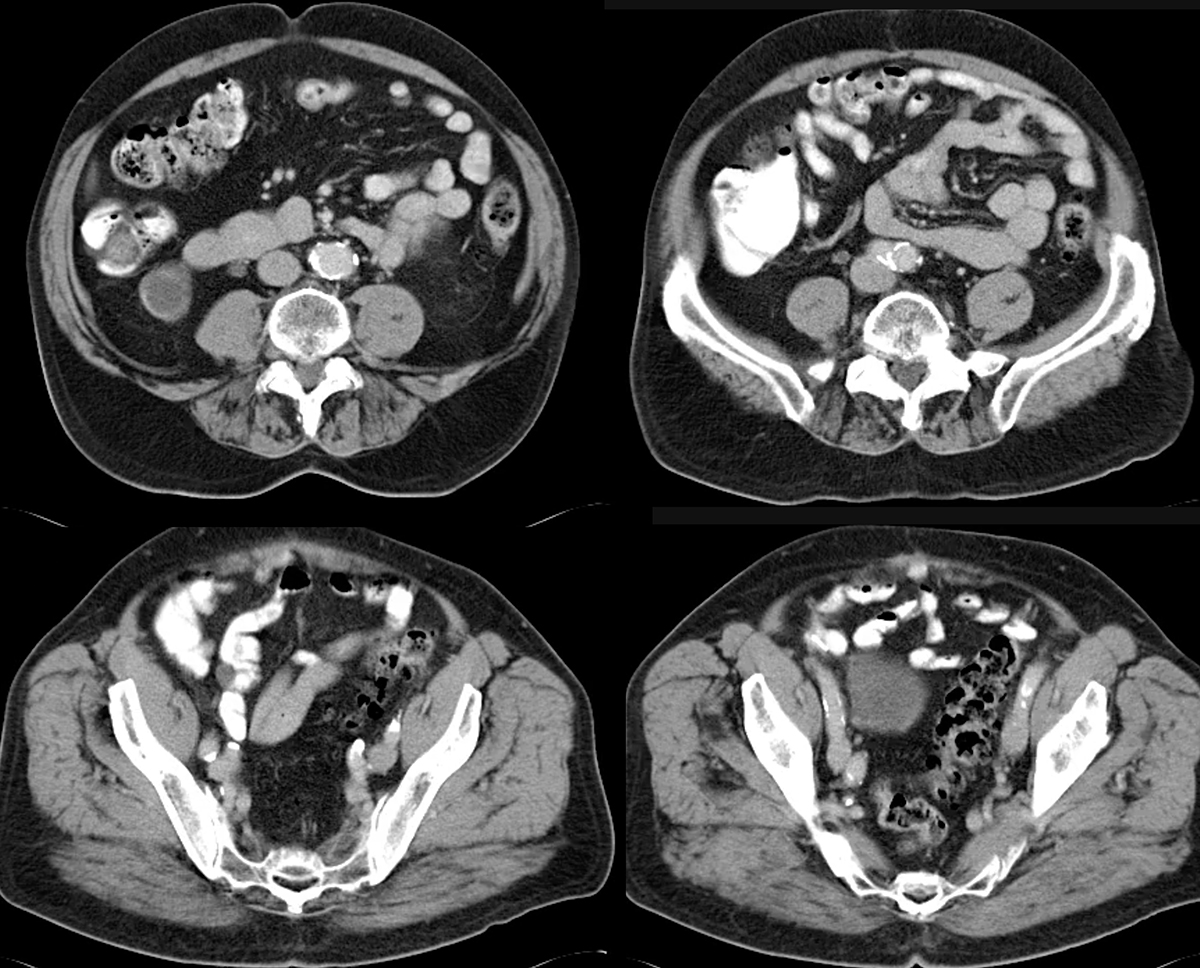
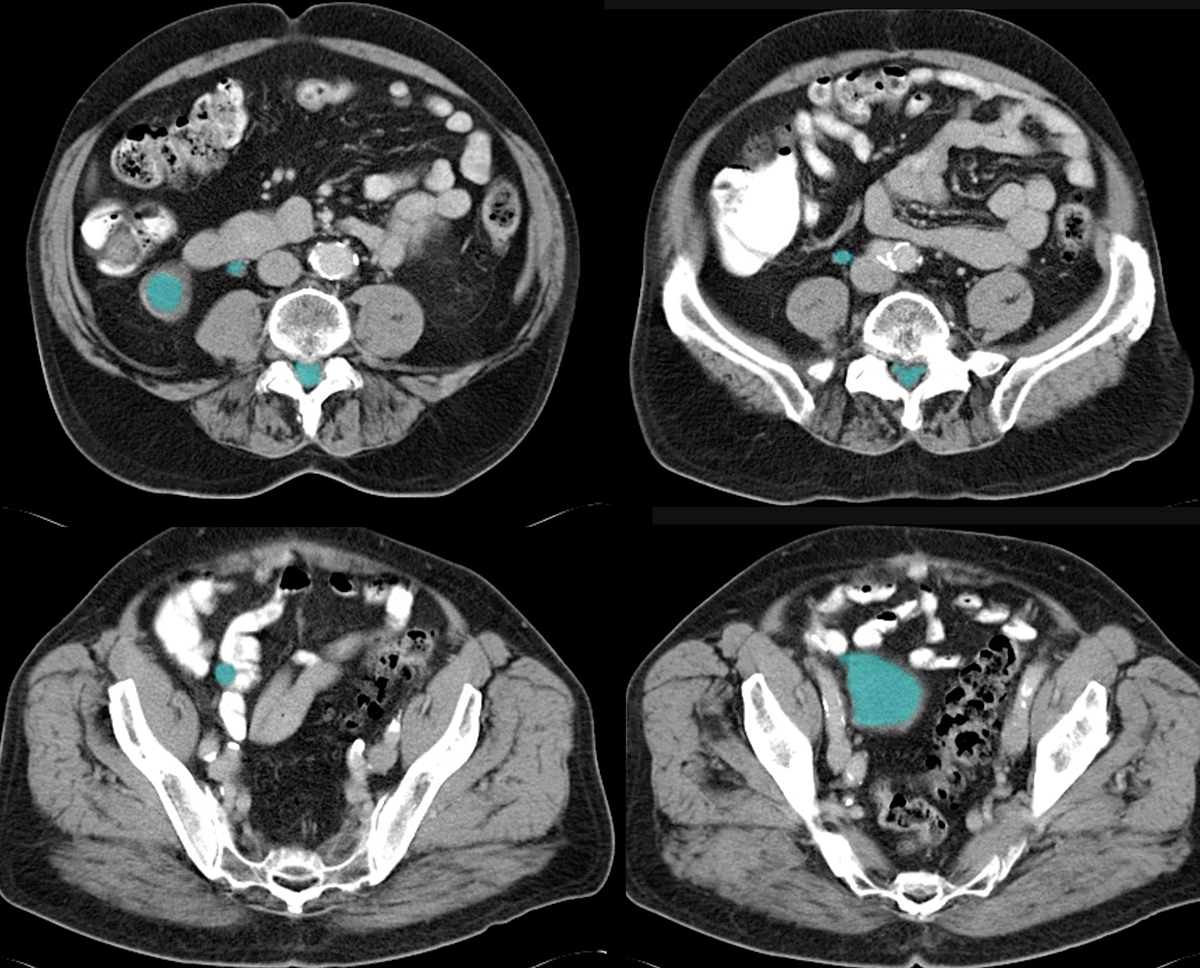
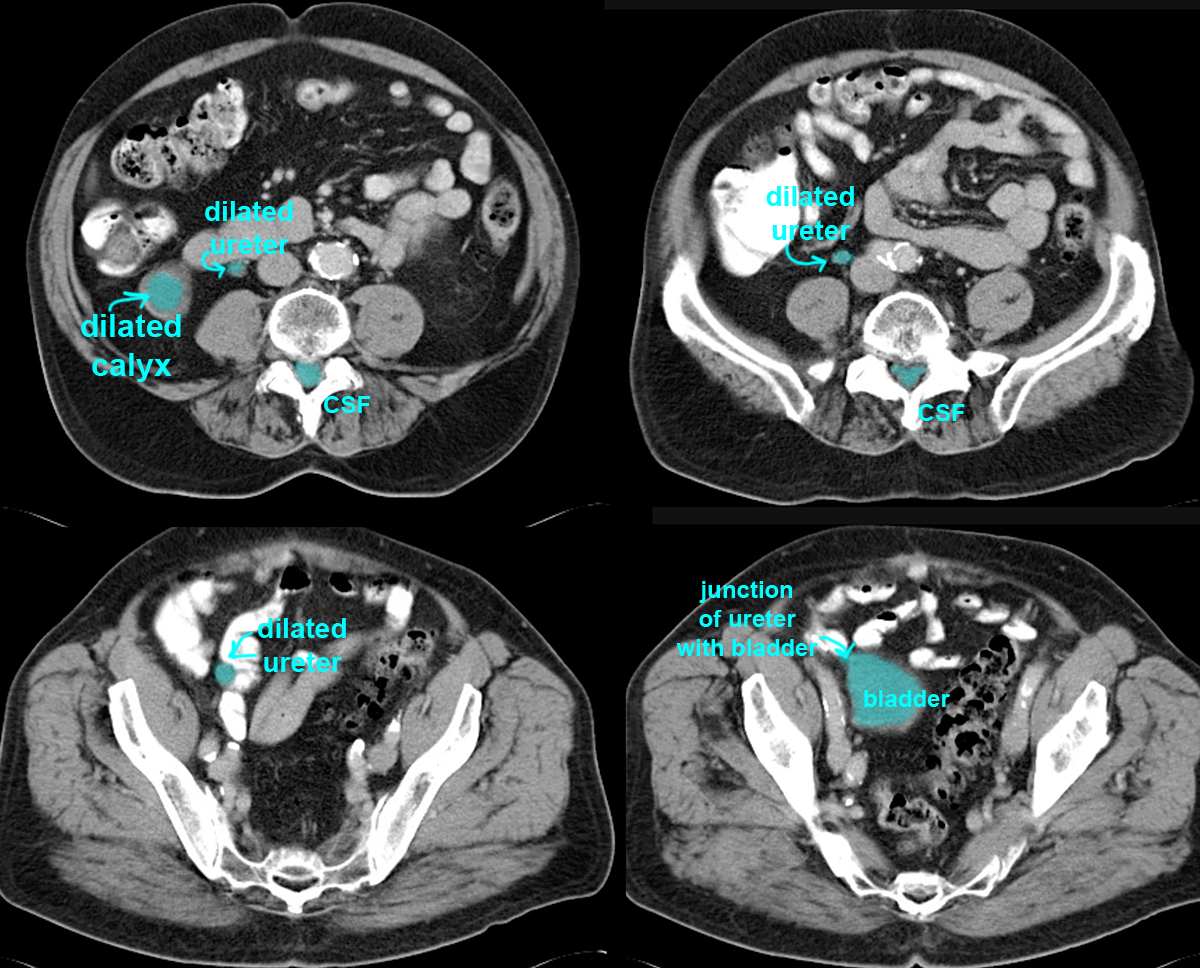
d) Given the appearance of the ureter on the right, indicated below, where is the likeliest point of obstruction?
Since the ureter is dilated all the way down to the region of its junction with the bladder, the point of obstruction was probably at the ureter-vesicle junction. No mass or stone is evident at this time, so it is possible that a prior stone eventually passed or was removed. Unfortunately, the obstruction went on long enough to produce a shrinkage of the right kidney, called 'atrophy'. This kidney likely is virtually non-functional now, but patients can usually do well with one normal kidney.
Abdomen Pelvis Case 3
This patient also has abdominal pain
Question 4:
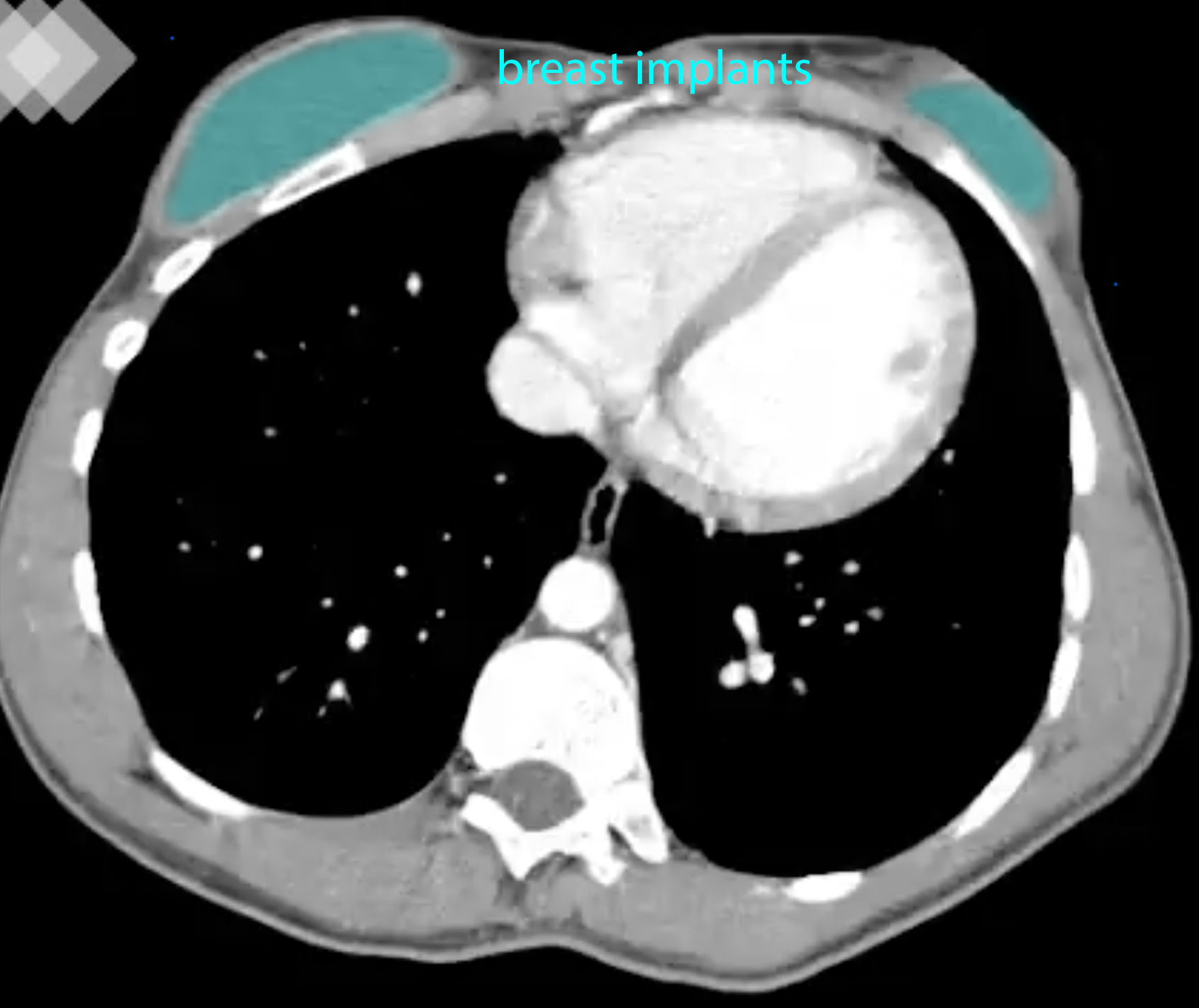
a) What do you notice on the uppermost images of this case when you search for fluid density? Are these the right windows to identify fluid optimally?
Click on the link below to show that she does have very well defined fluid collections just under the skin surface anteriorly, in the region of the breasts. The fluid has a very smooth margin, suggesting that it might be within a foreign object--these are breast implants, filled with saline. These are soft tissue windows, which are ideal for visualizing fluid and recognizing that its density is different from muscle.
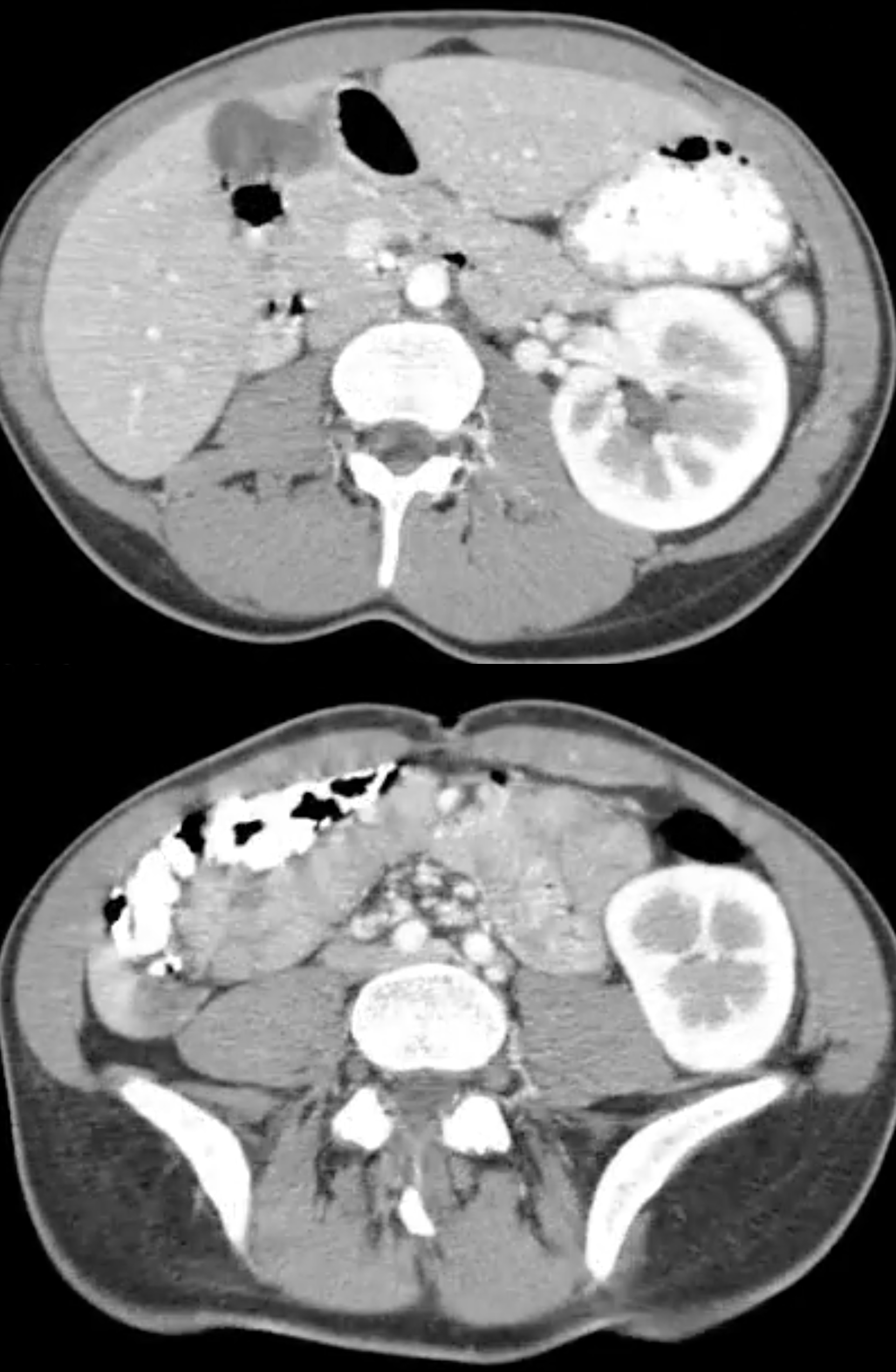
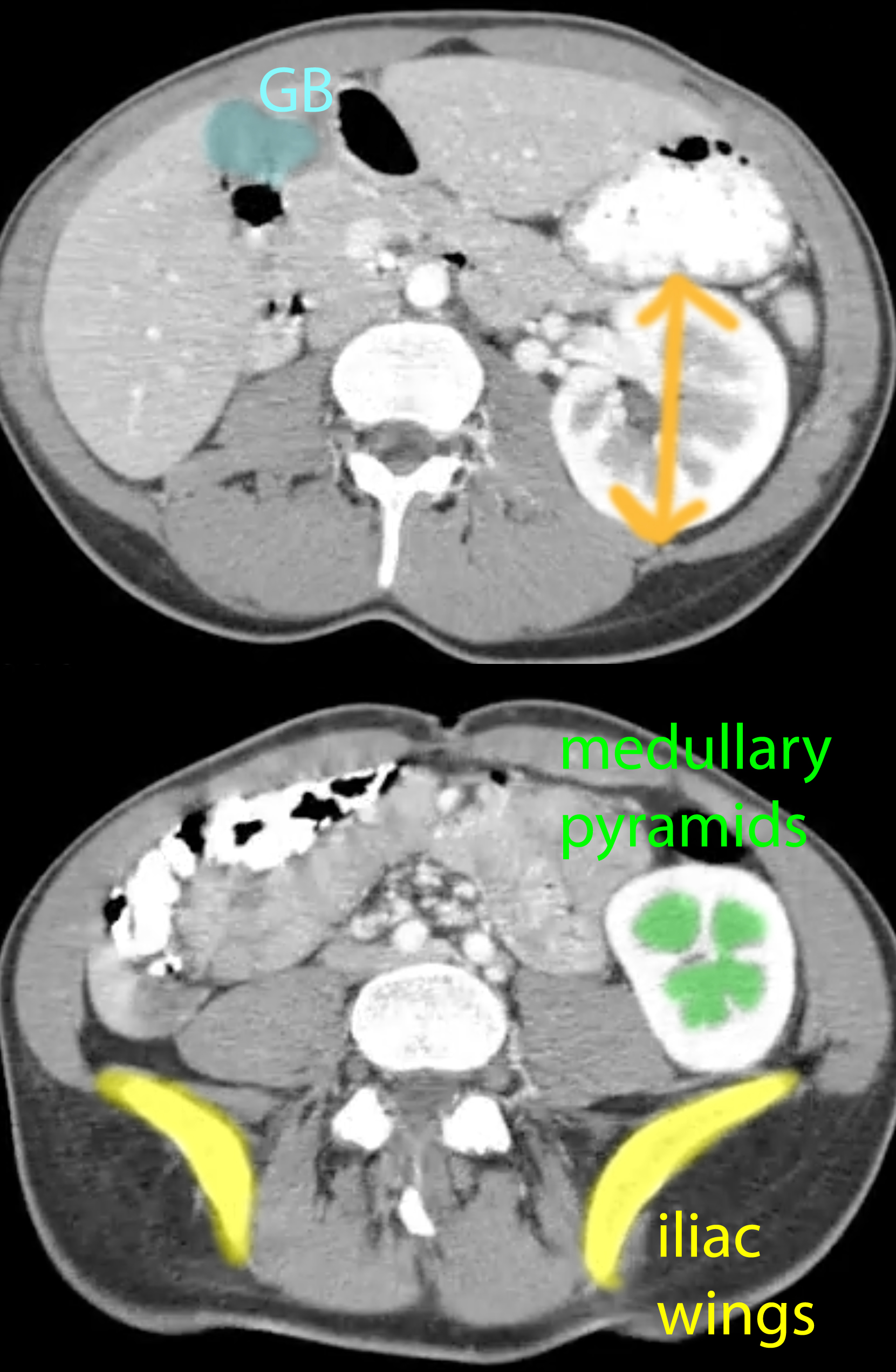
b) What is abnormal about the kidneys in this patient, and what other imaging plane might be useful to examine?
There are not kidneys, but one single kidney, on the left. As previously mentioned, the kidneys initially develop in the pelvic region and migrate upward to their normal final position but sometimes things can go wrong. Kidneys can stay in the pelvic region, or can fuse in the midline (a horseshoe kidney). Sometimes, as in this patient, one of the embryologic precursors may not develop, leaving only one kidney. In this case, the single kidney is often larger than a normal kidney, as it has taken over the function of the other missing kidney. If you look at the kidney images below, you can appreciate that this kidney extends from the upper abdomen(where the gallbladder is) into the pelvis, which is not the normal size of a kidney. Coronal images would be useful to evaluate the top-to-bottom length of the kidney. The marked difference between the contrast enhancement of the renal medulla from the cortex shows that this study was performed in the early phase of contrast enhancement.
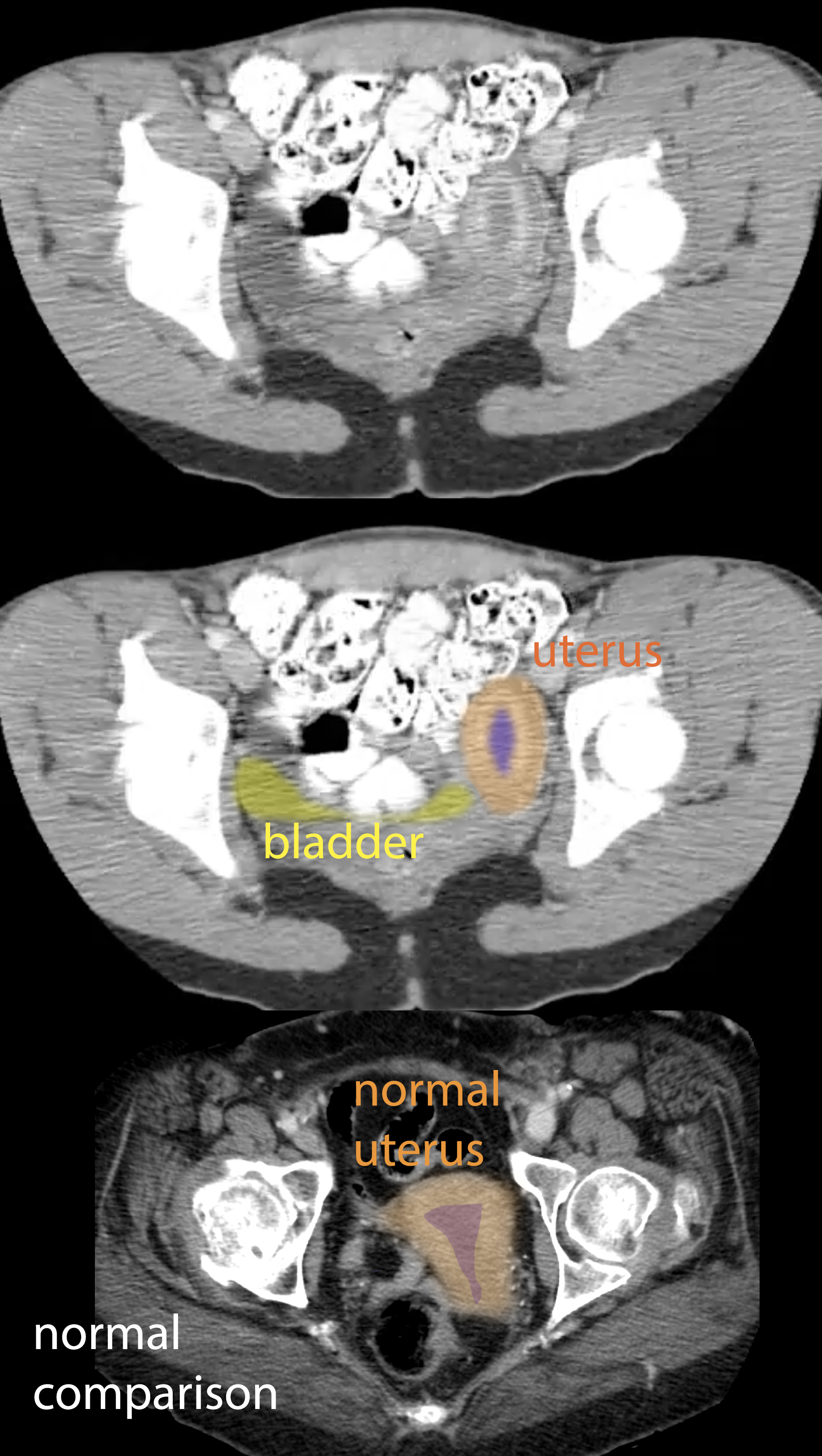
c) If the precursor embryologic structure that forms the kidneys was abnormal in this patient, what other system might be affected?
The kidneys and the genital tract share a common embryologic precursor, so if a patient has only one kidney, it is important to look at the genital system as well. If you look at the images of the uterus below, you can see that there is a strange tubular shape to the uterus, which is far to the left in position. This is because only half of the uterus developed, producing what is called a unicorrnuate, or tubular-shaped uterus.