Case 4-low back pain
Low back pain (LBP) is a very common cause of primary care visits, and can be quite debilitating. While imaging is often performed, it is important to realize that the correlation with imaging and symptoms is often not helpful. Imaging can play an important role in excluding some causes of LBP, such as tumors, fractures or infections. But the sensitivity and specificity for other causes of LBP, such as strain or disc disease is often low.
Question 1:
a) What types of imaging can be done for LBP evaluation?
Everything from radiography to ultrasound, MRI to nuclear medicine and invasive procedures like myelography can all play a role in imaging LBP. However, no imaging at all may be the correct answer if there are no serious accompanying symptoms such as neurological deficits. Often radiographs are obtained first as they can exclude some serious conditions, are fast and cheap to perform, but have a very low sensitivity for many causes of LBP. You are shown a set of normal lumbar spine radiographs below to review the pertinent anatomy.
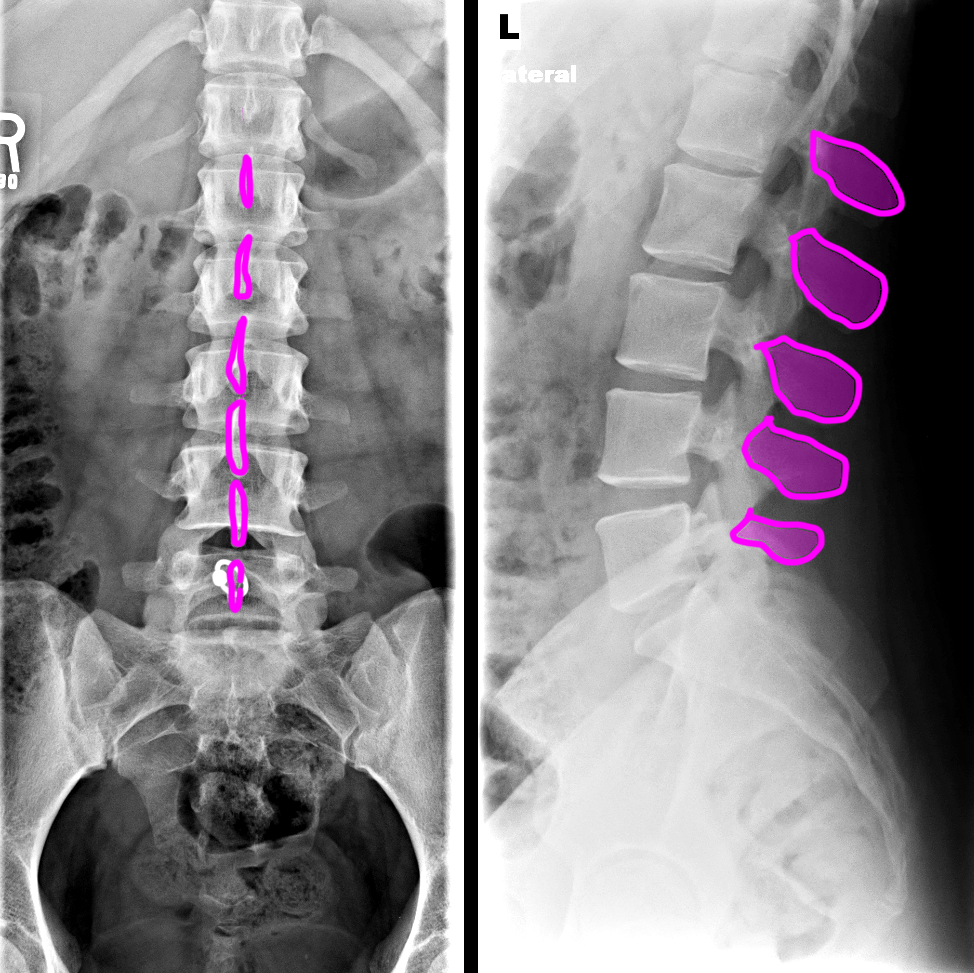
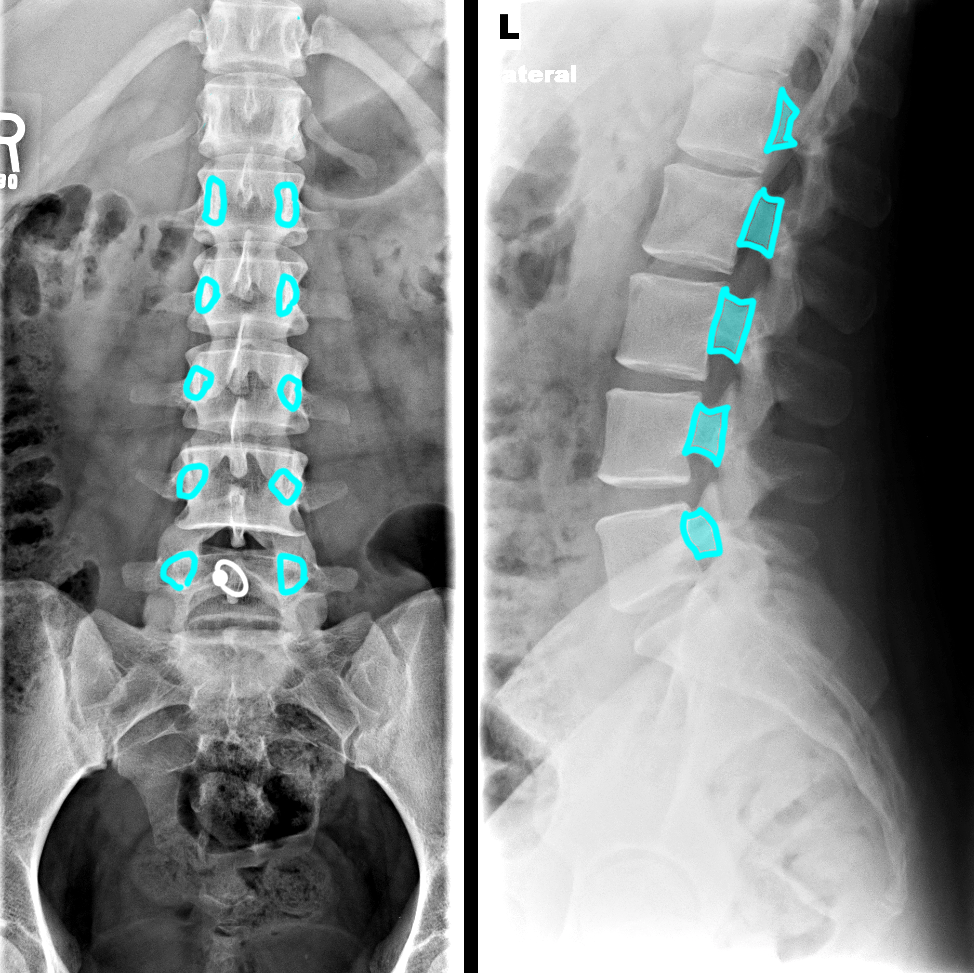
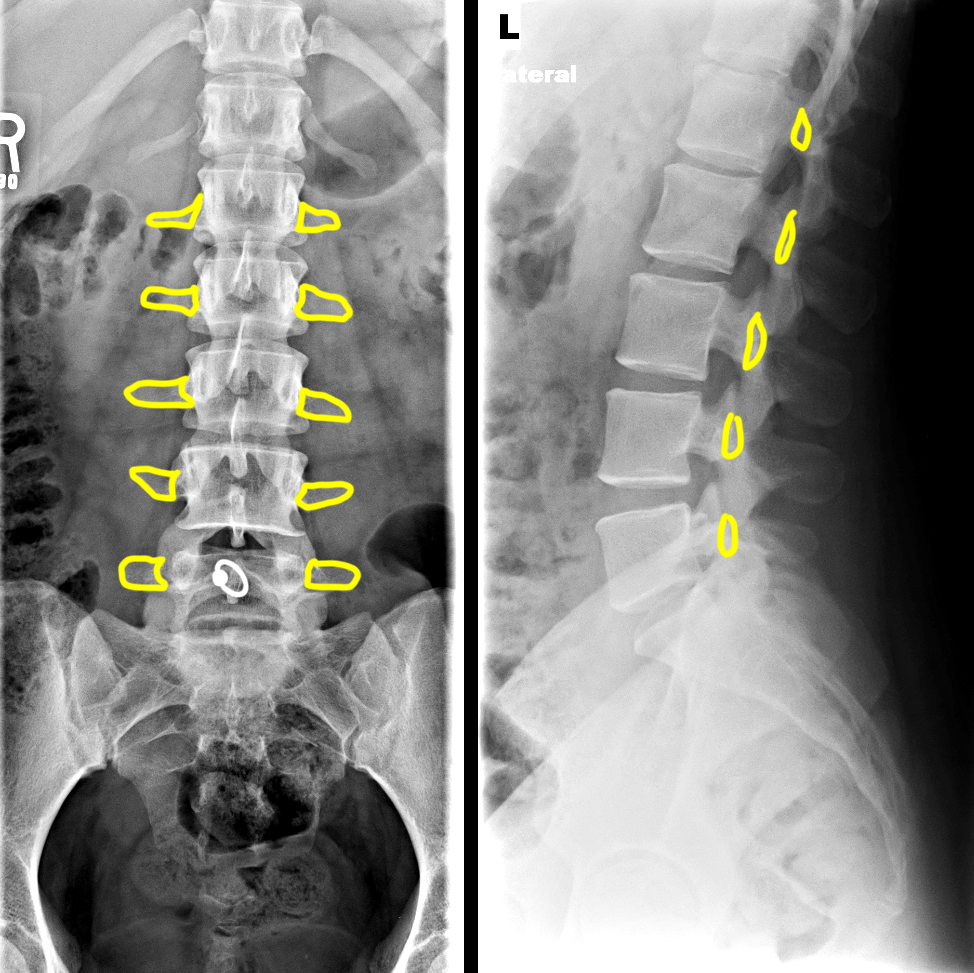
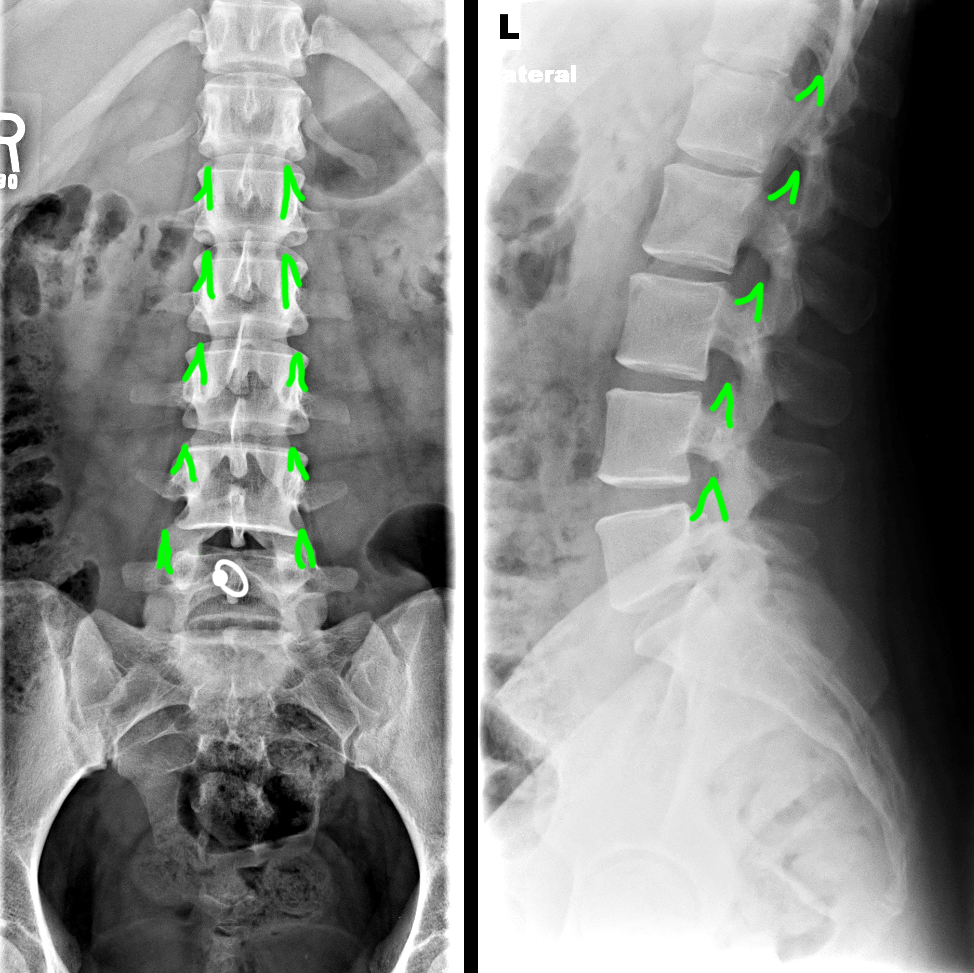
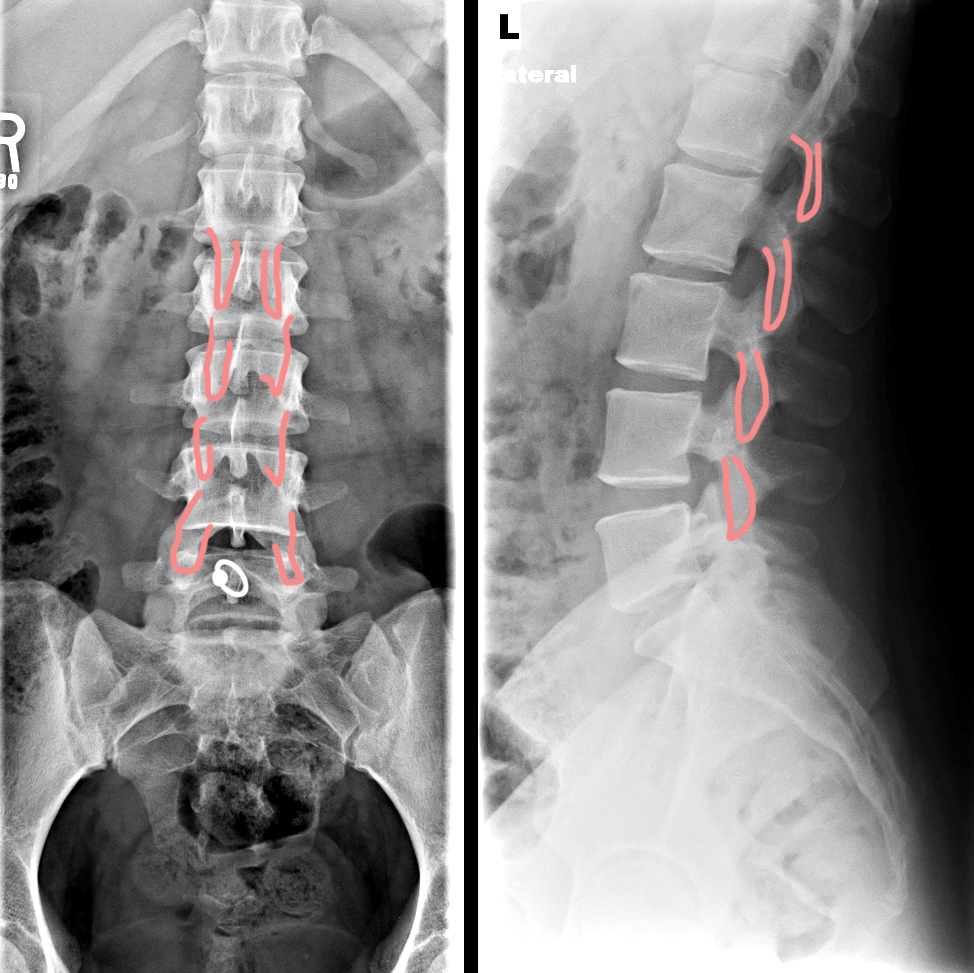
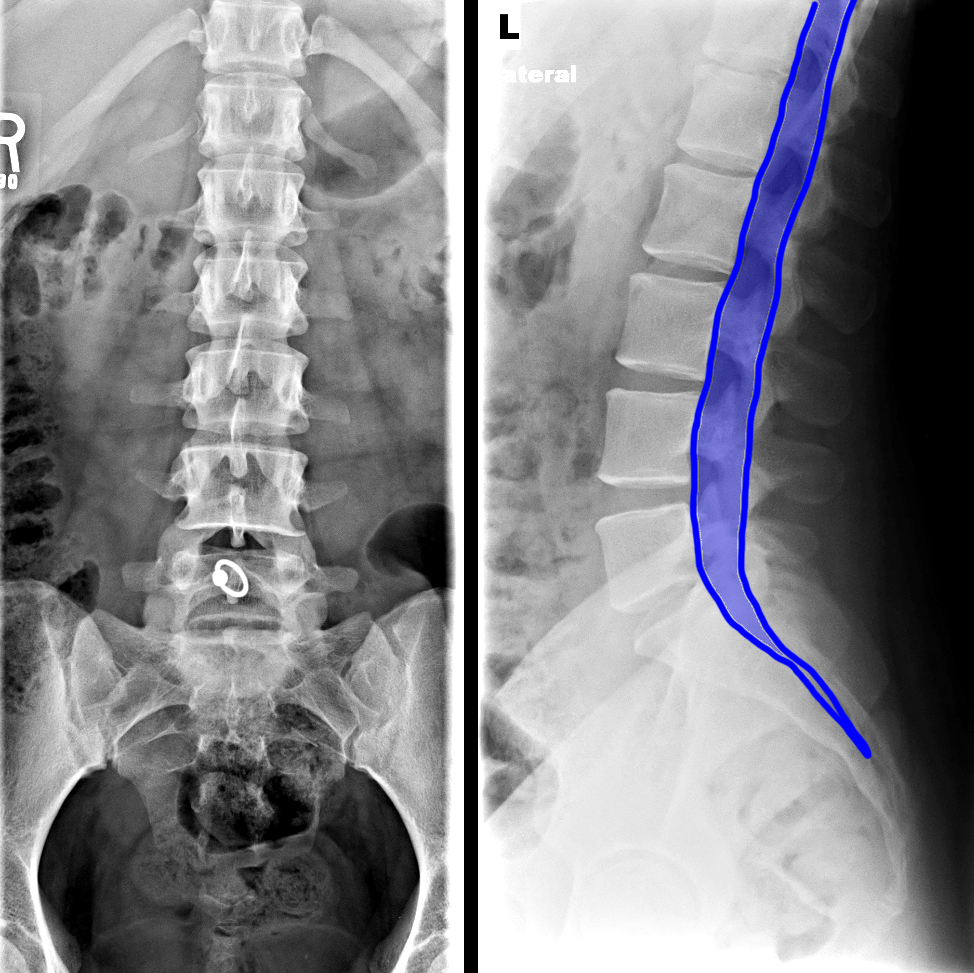
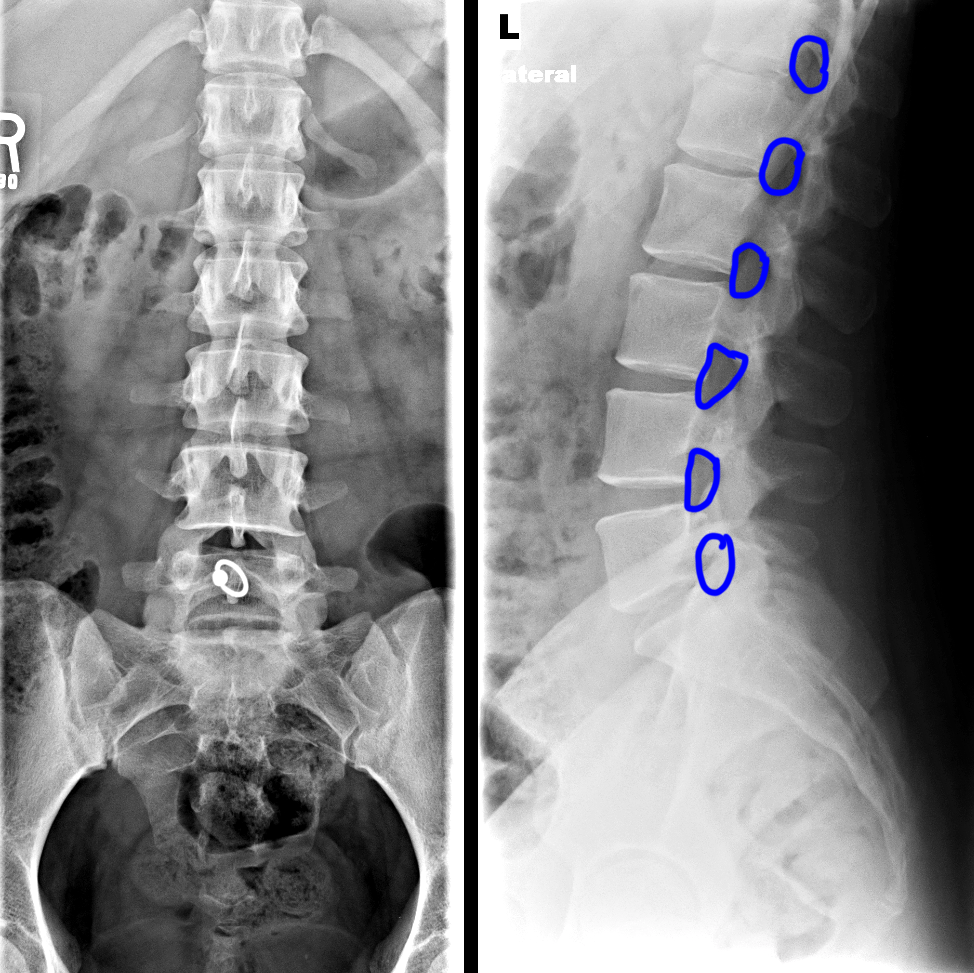
b) What are the lumbar spine structures shown below?
1-spinous processes; 2-pedicles; 3-transverse processes; 4-superior articular facets; 5-inferior articular facets; 6-spinal canal (containing spinal cord and nerve roots); 7-neural foramina (from which nerve roots exit)
Case 4-low back pain
While no imaging initially may be the correct management for many cases of LBP, if worrisome symptoms are noted or if the pain persists, then imaging may be needed. You are shown two examples of more invasive imaging of the lumbar region.
Question 2:
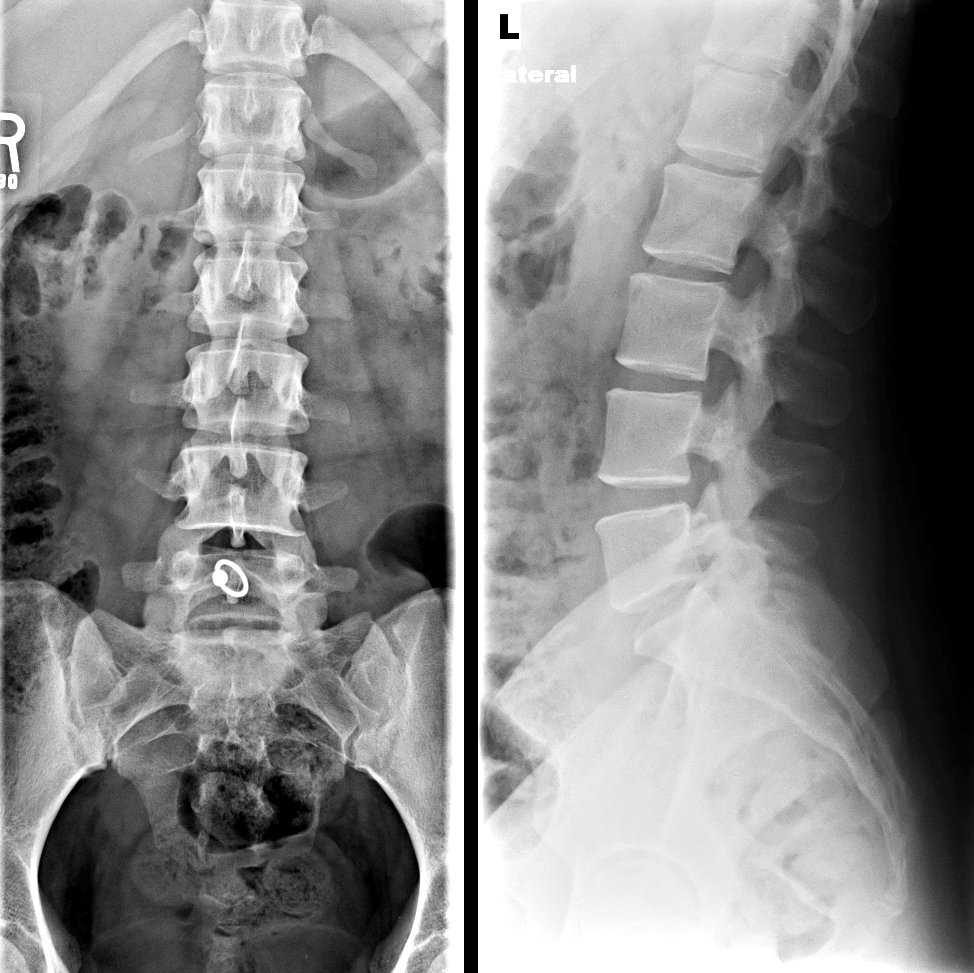
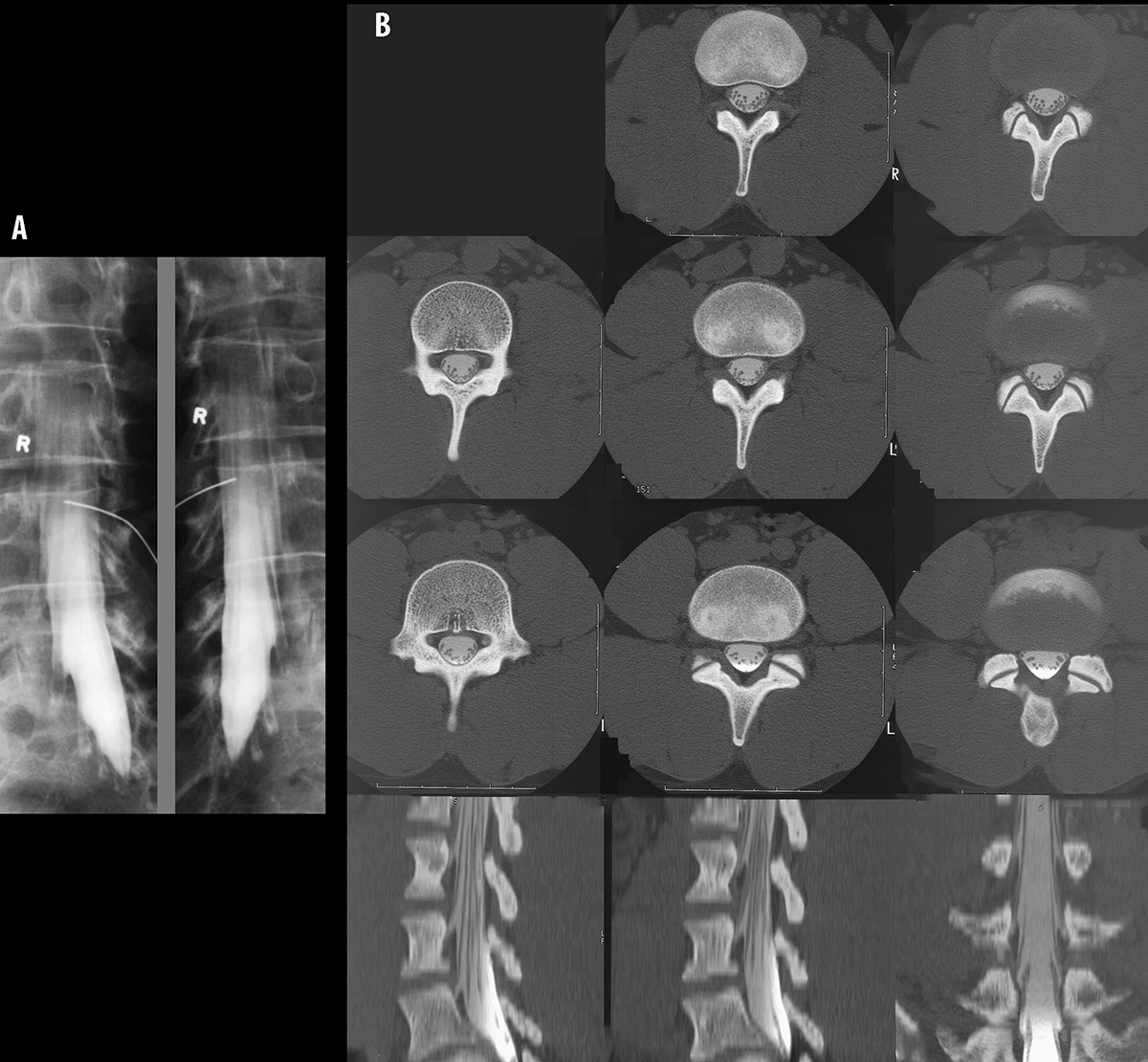
a) What are these two studies, and what do they have in common?
Image A is a lumbar pyelogram, and Image B is a CT myelogram. In both cases, a lumbar puncture is performed and contrast is introduced into the CSF space. For the myelogram, radiographs are then performed in various projections. For the CT study, a CT scan is performed.
b) Is the spinal cord visible on either study?
No. Both studies are focused on the lower lumbar regions, and only show the cauda equina, or the nerve roots heading downward from the cord, which typically ends at about the L1 or L2 vertebra.
Case 4-low back pain
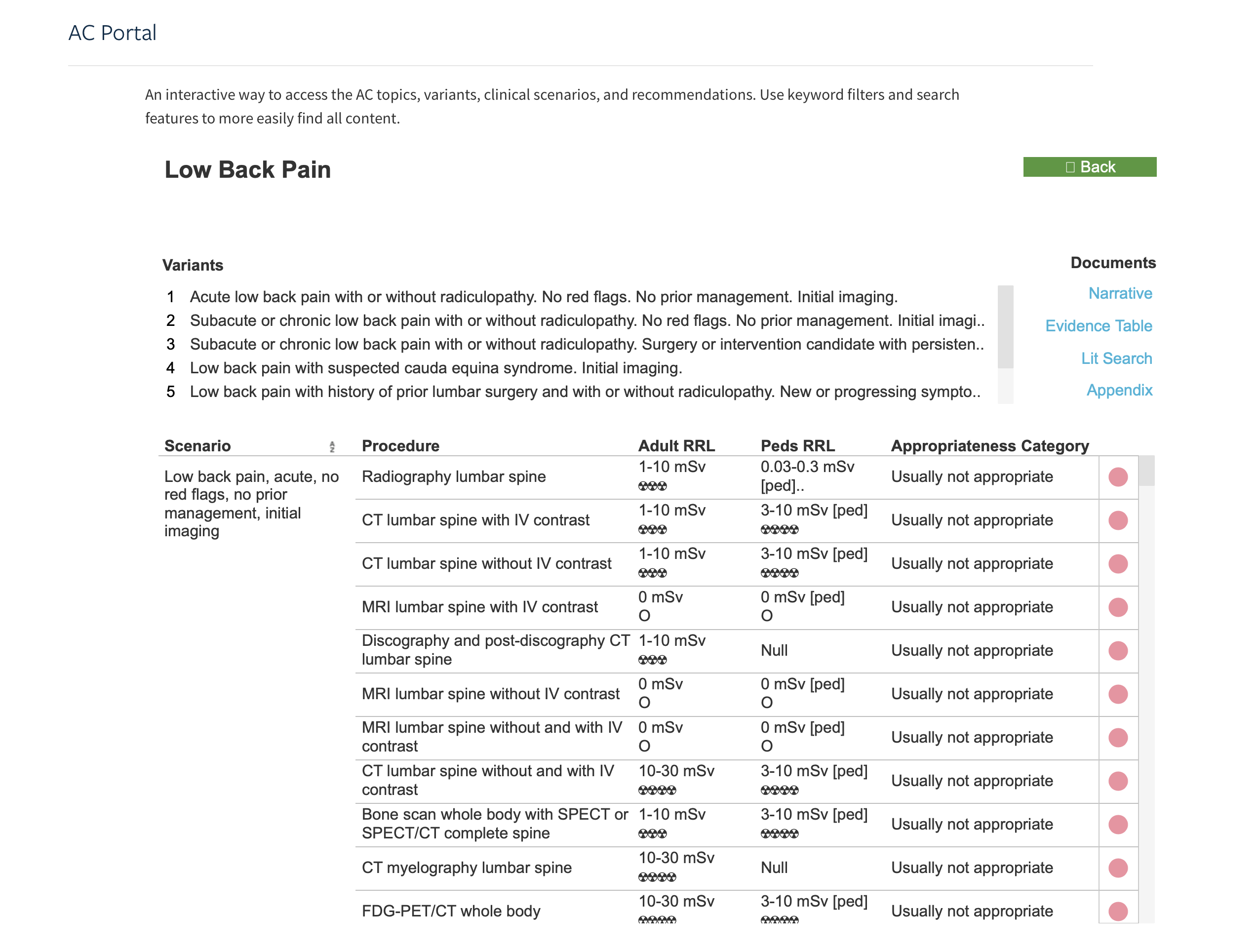
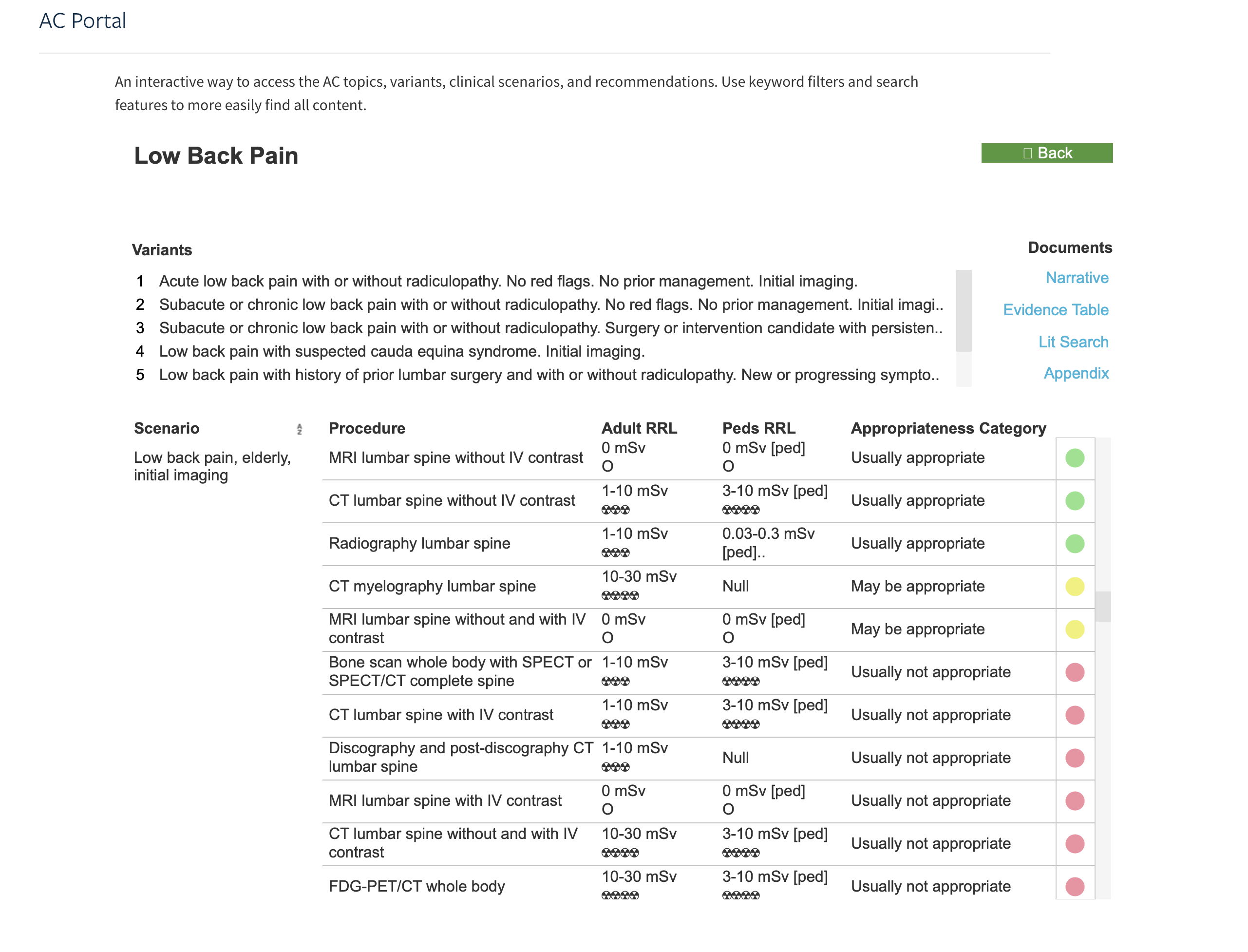
Another common way to image the lumbar spine is with MRI. MRI shows cartilage, discs, and neural structures better than radiography or CT. However, findings on MRI (such as bulging discs) do not always match exactly with patient symptoms. Sample information from the ACR Appropriateness website for two LBP scenarios are included.
Question 3:
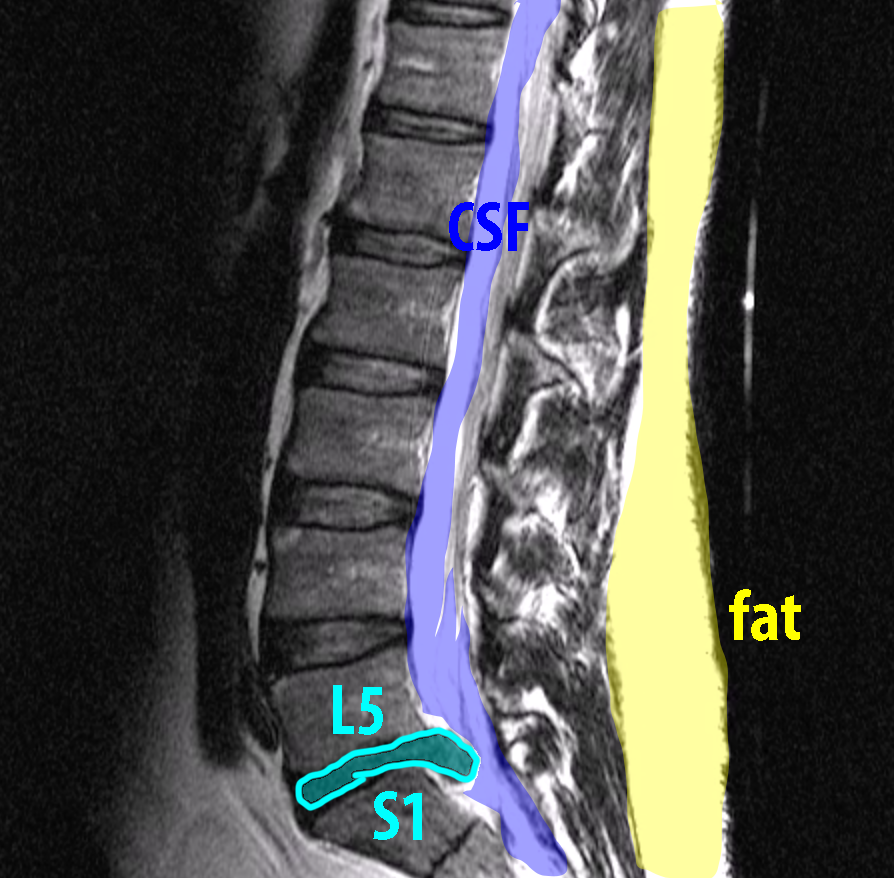
What are the technical parameters for this study, and at what level is there an abnormal disc?
This study is a sagittal T2 weighted MR without fat supression. The fluid in the CSF space is high signal and so is the subcutaneous fat. There appears to be a protruding disc at the L5-S1 level. Whether this correlates with the patient's symptoms should be confirmed before considering treatment.