Case 3-other imaging
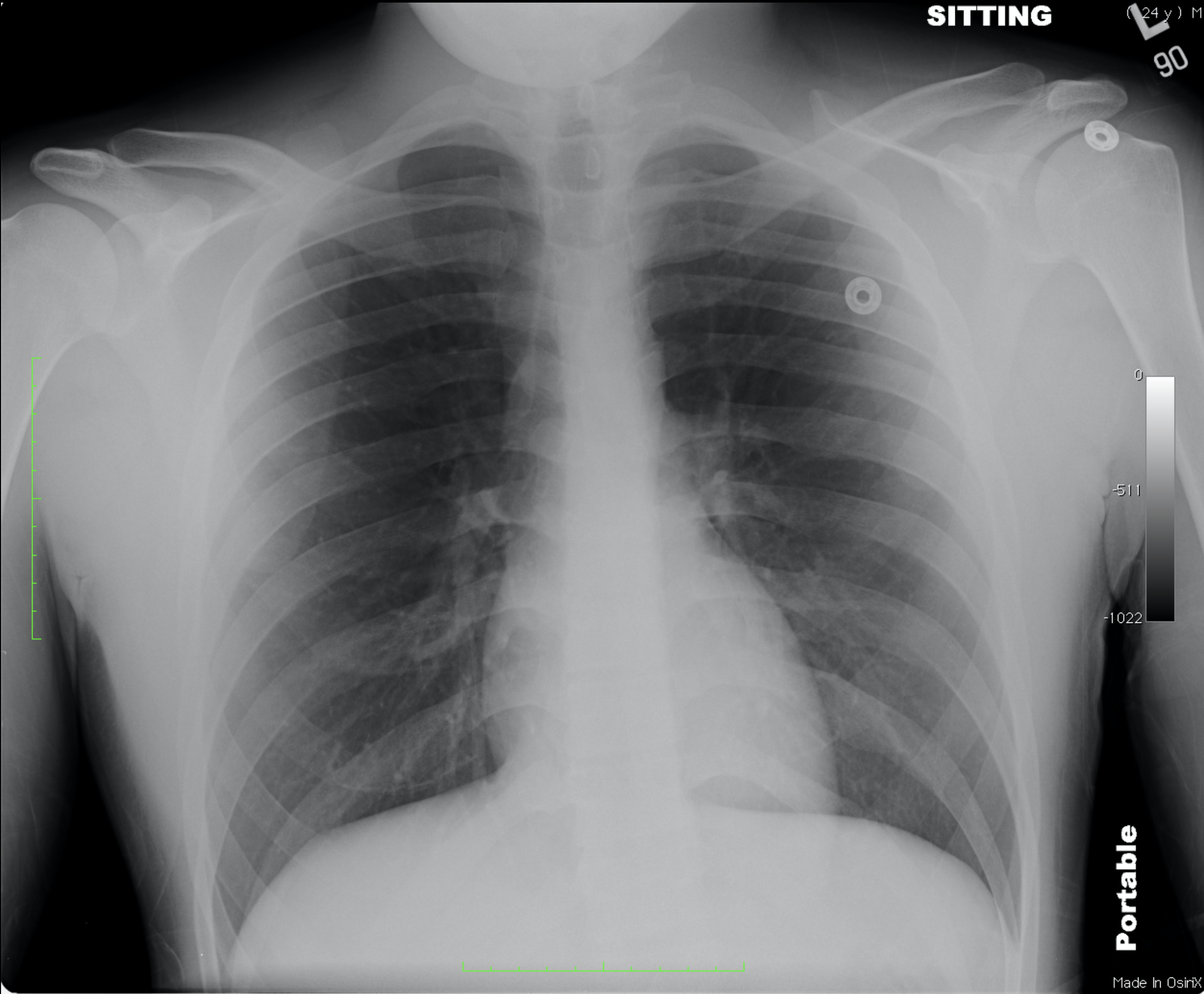
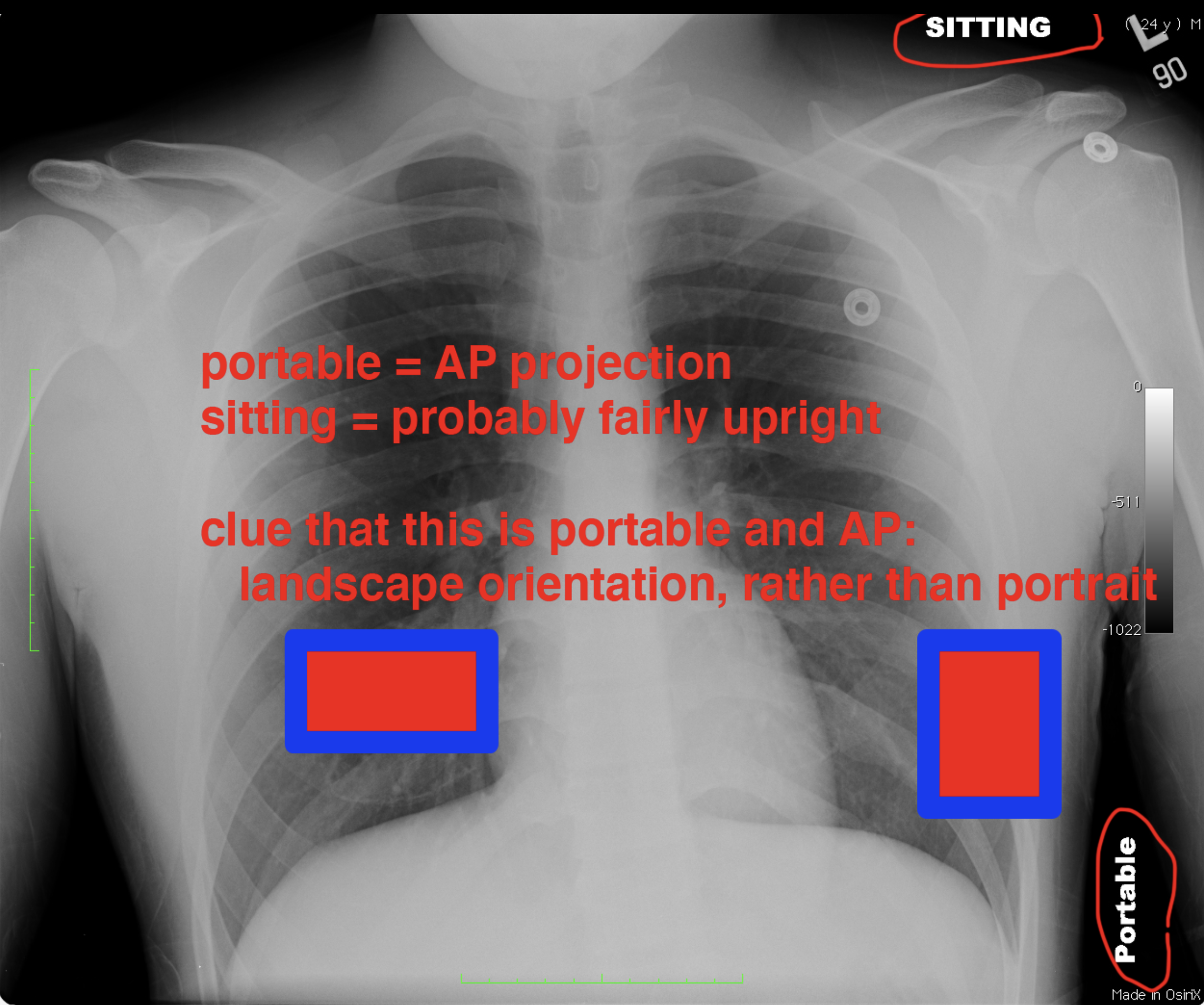
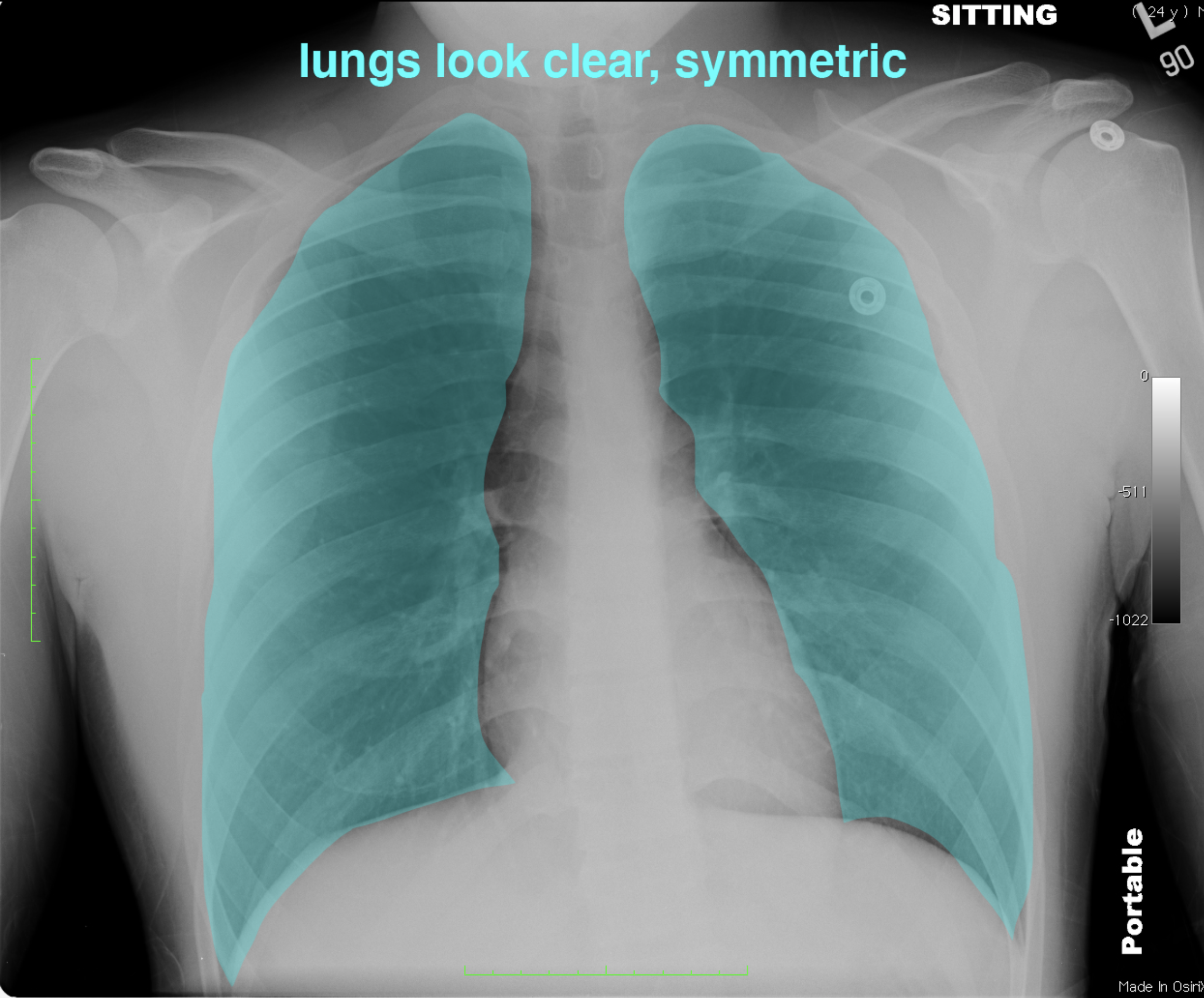
This is a different type of chest radiograph, a portable study. While portable studies can be done in various positions, most often the patient is supine or semi-erect and the image is performed in the AP projection (which can lead to magnification of the apparent heart size). Ideally, there should be a marker or label to indicate the patient position.
Further Explanation:
Case 3-other imaging
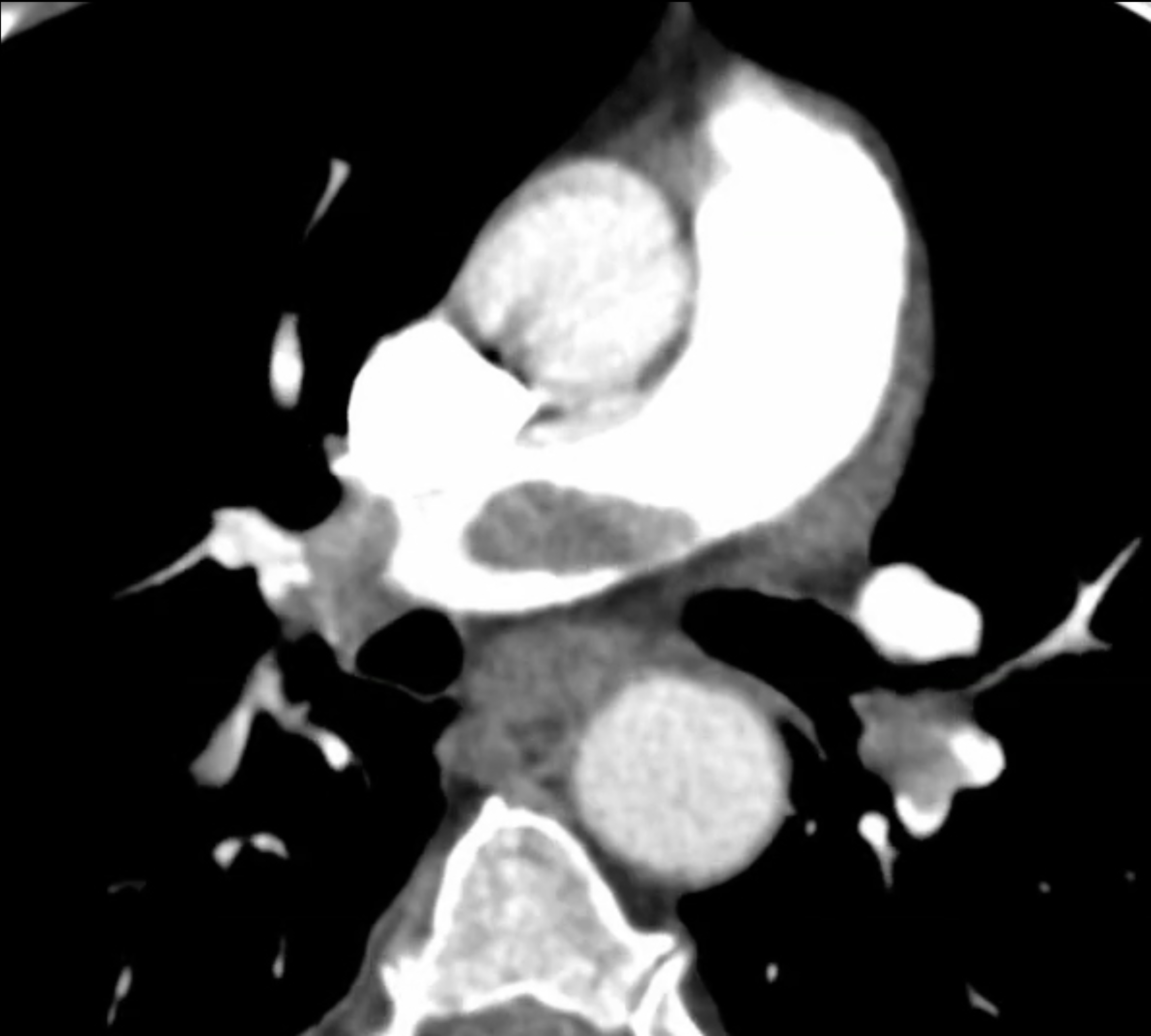
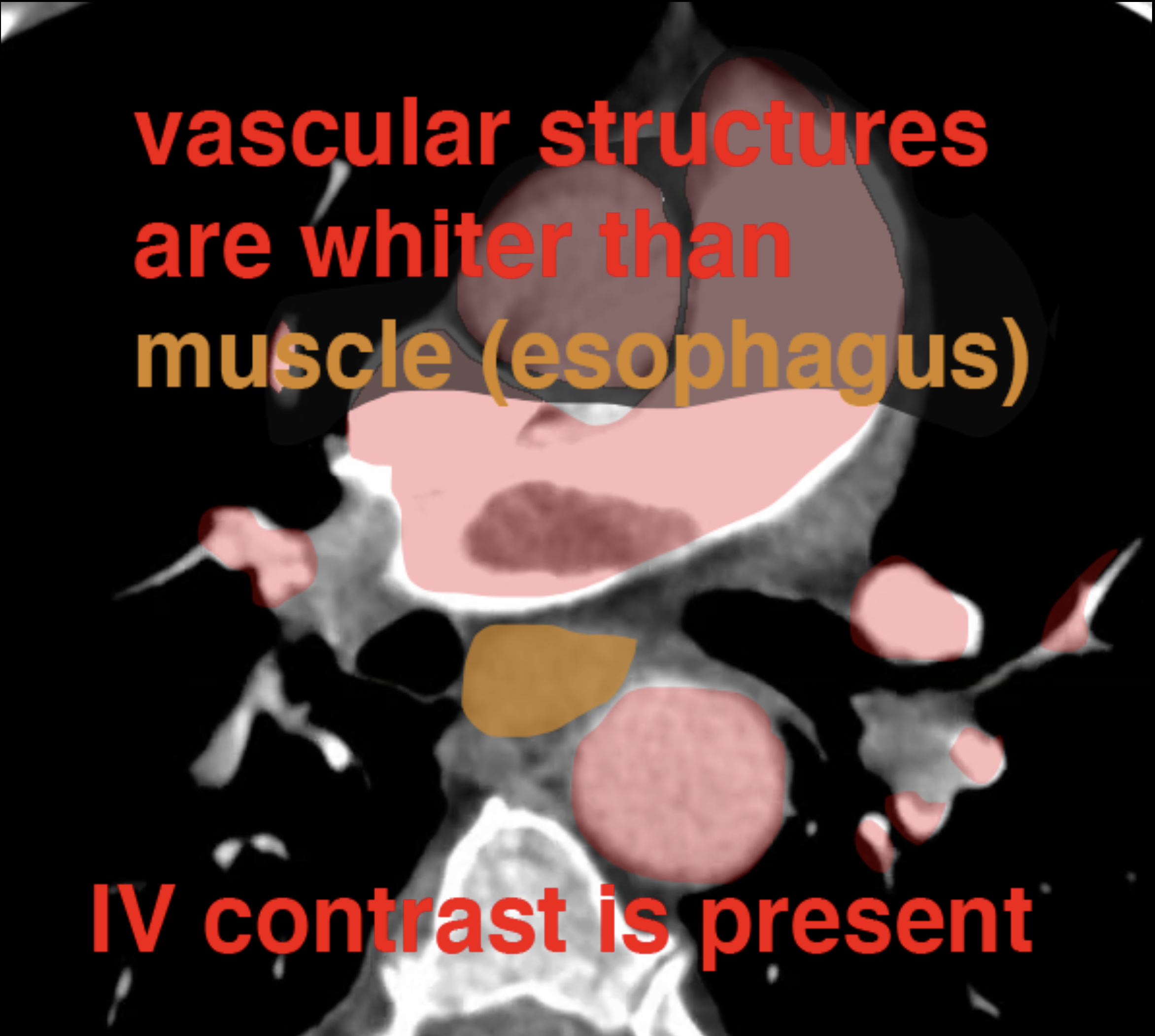
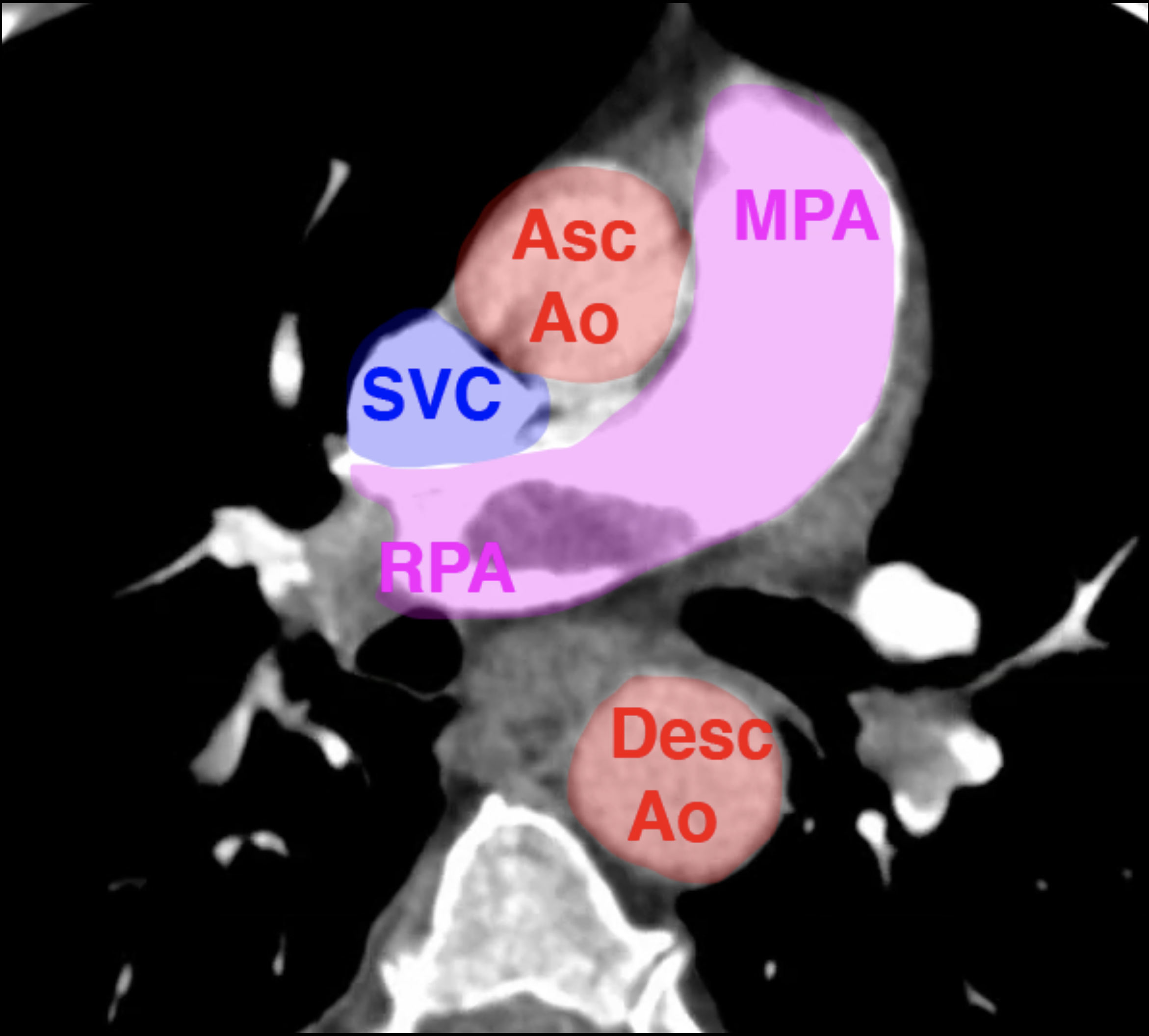
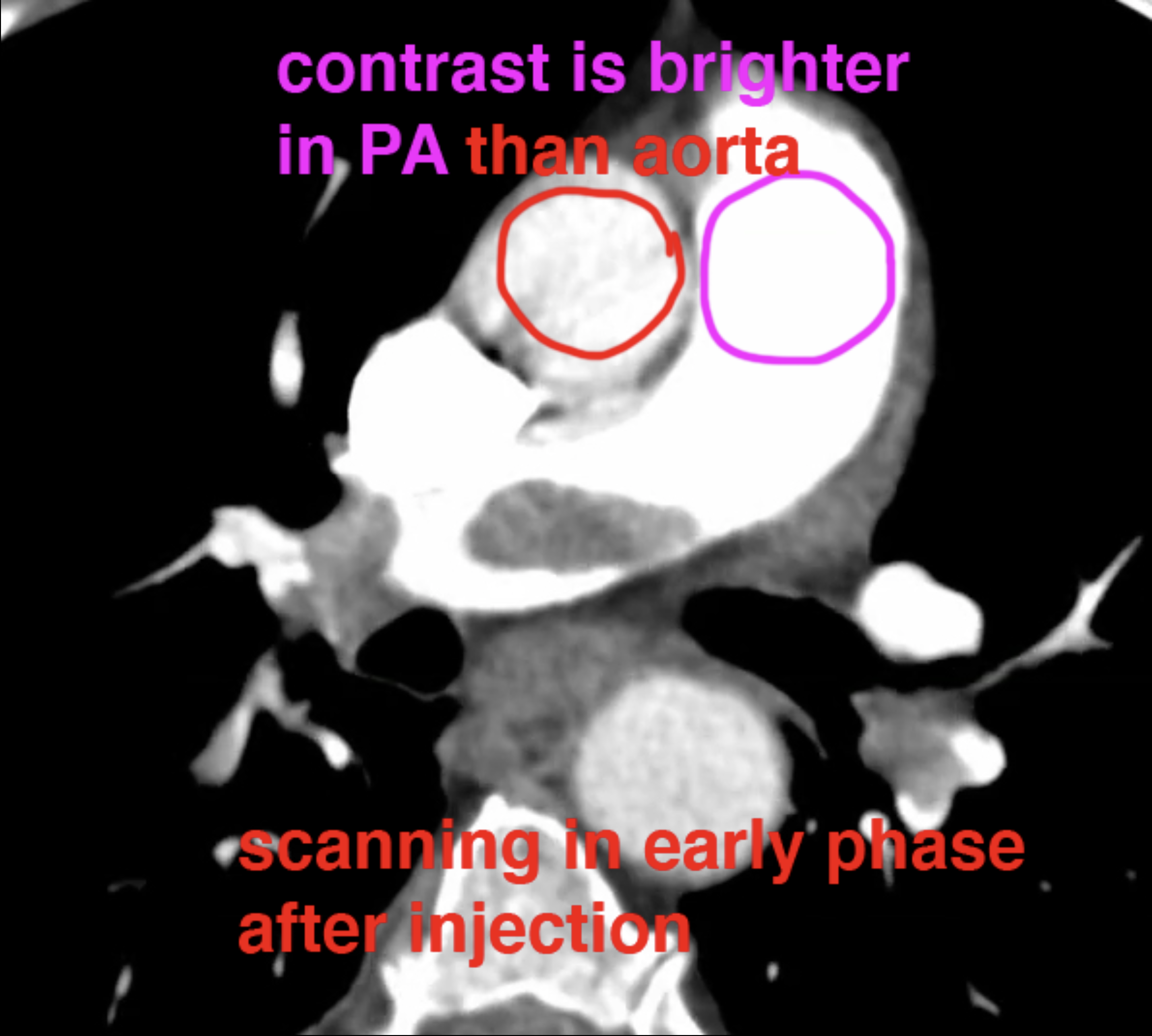
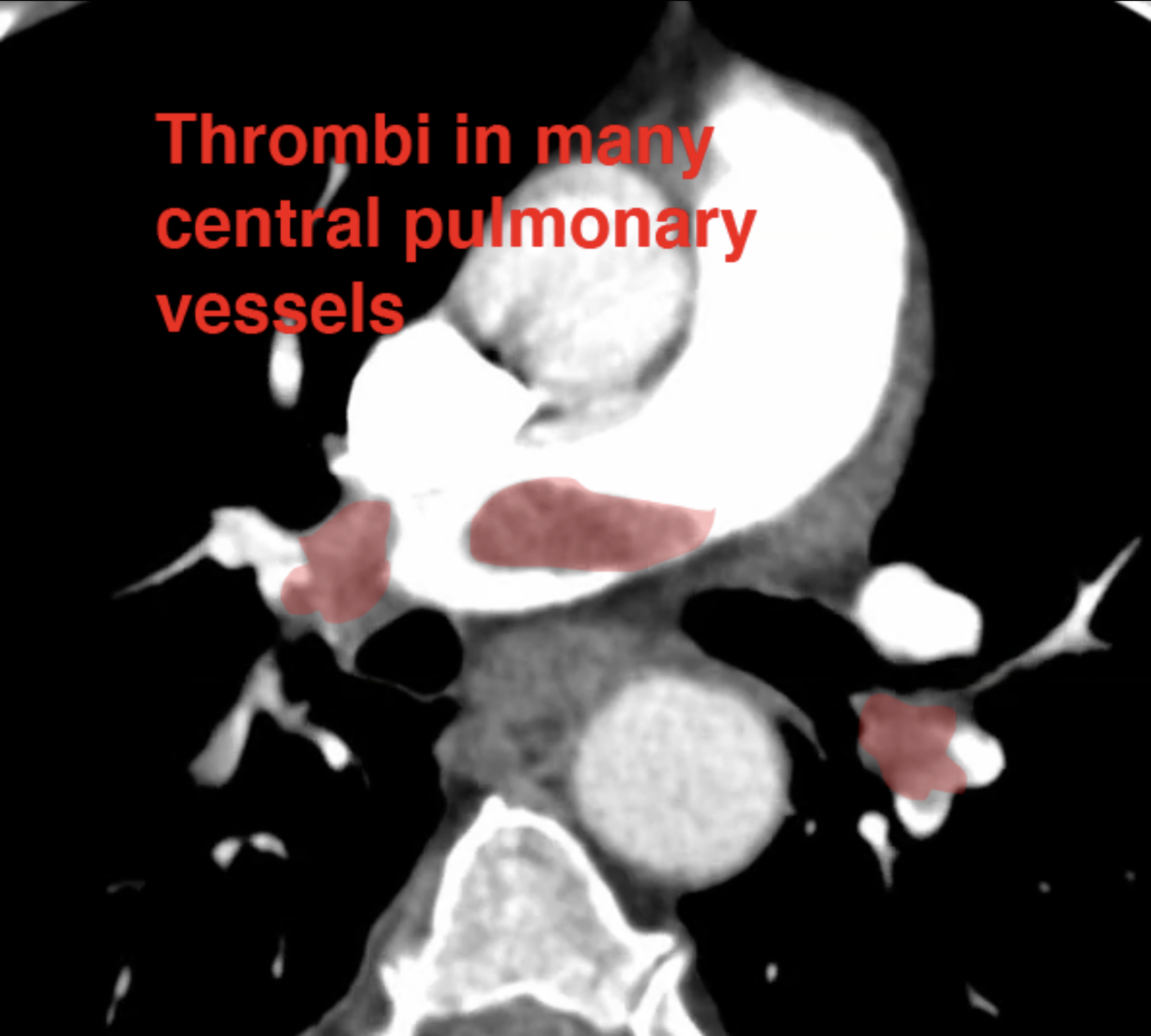
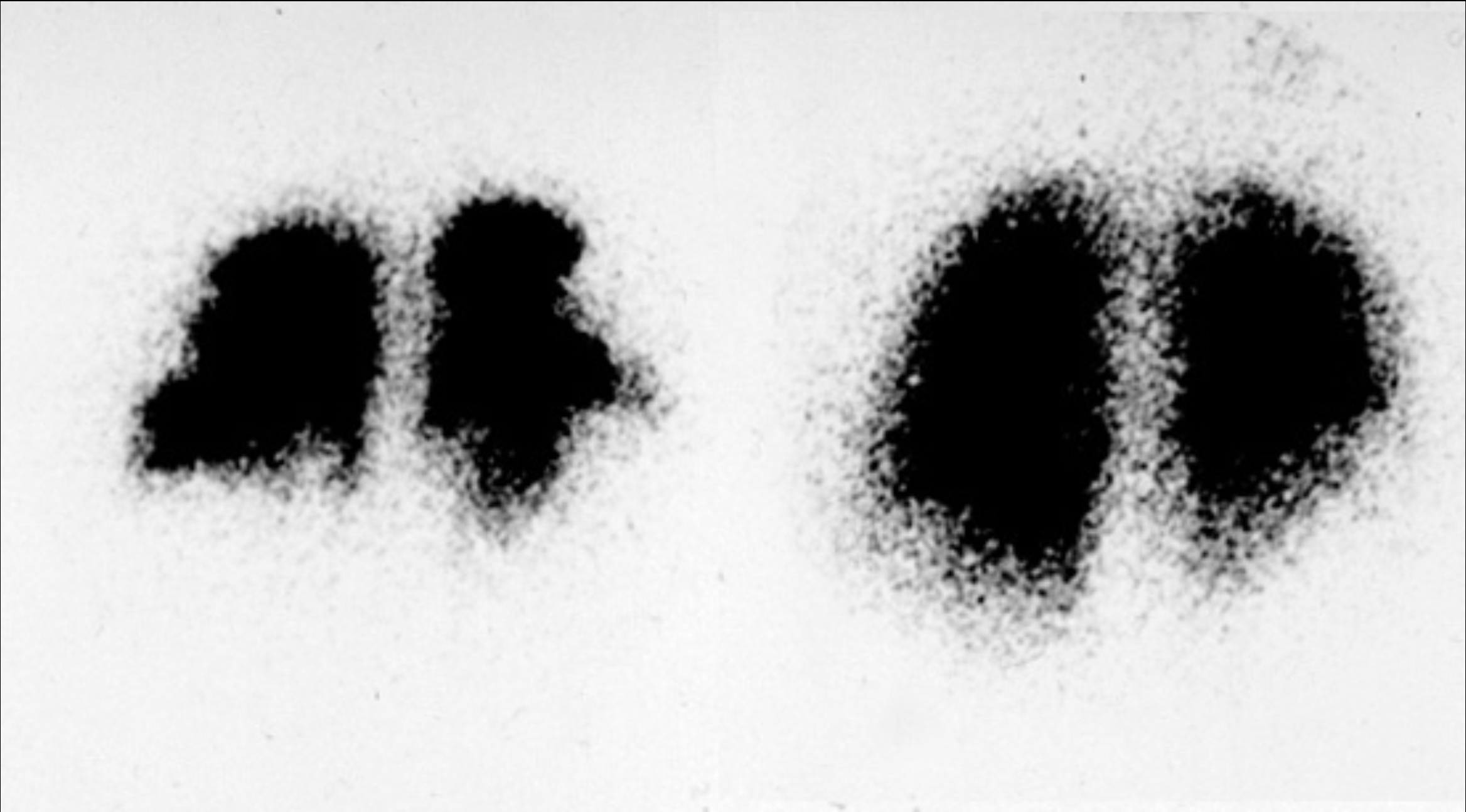
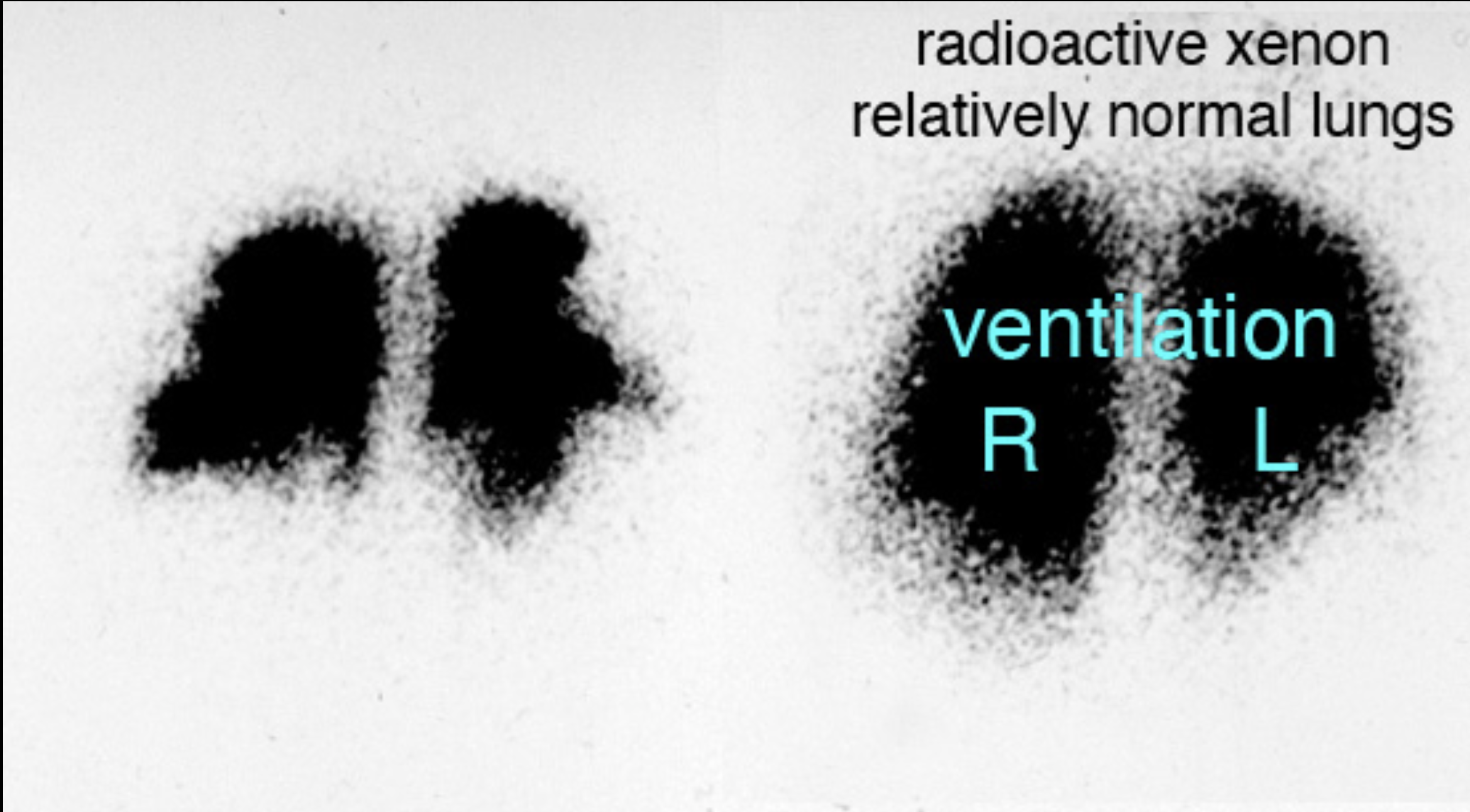
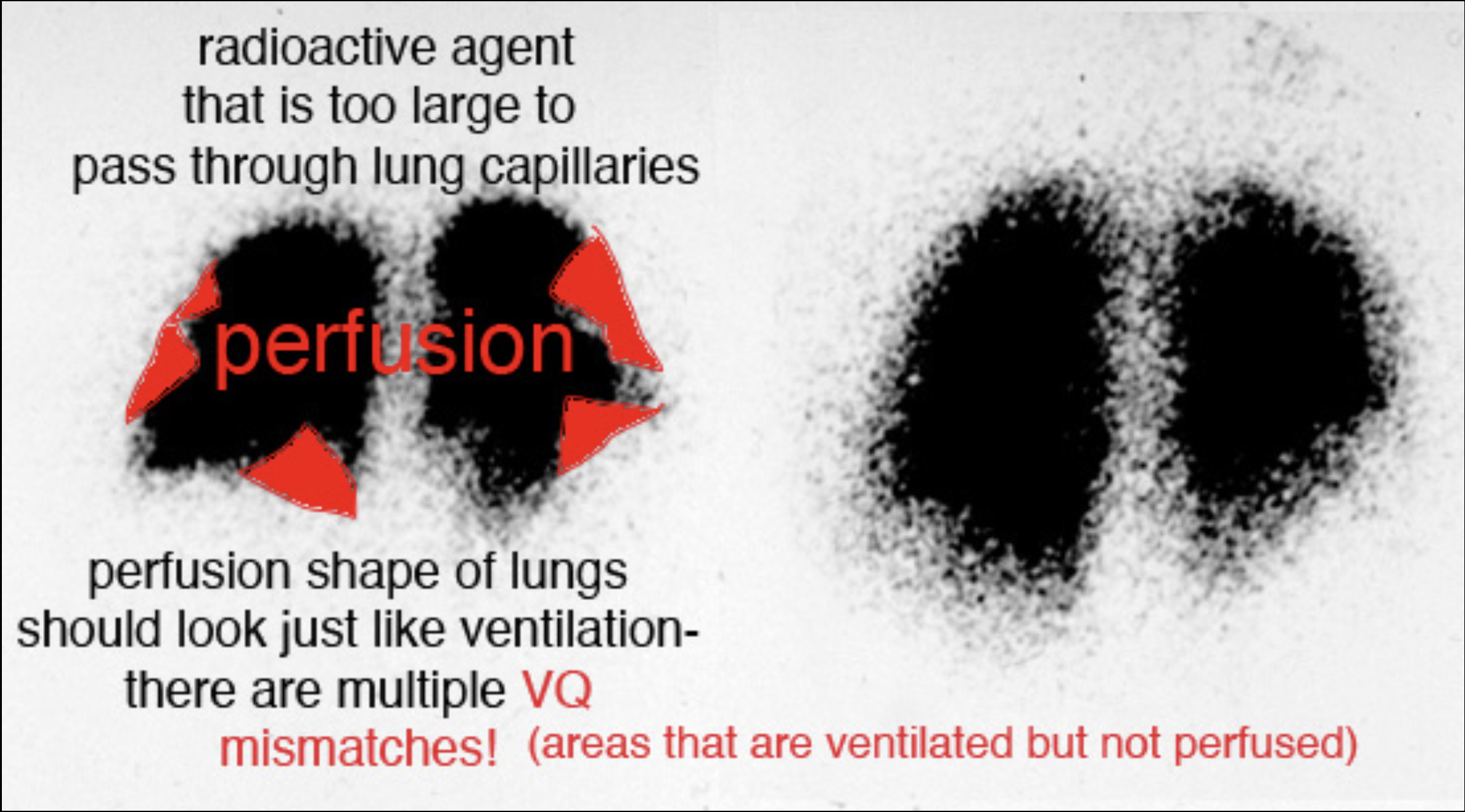
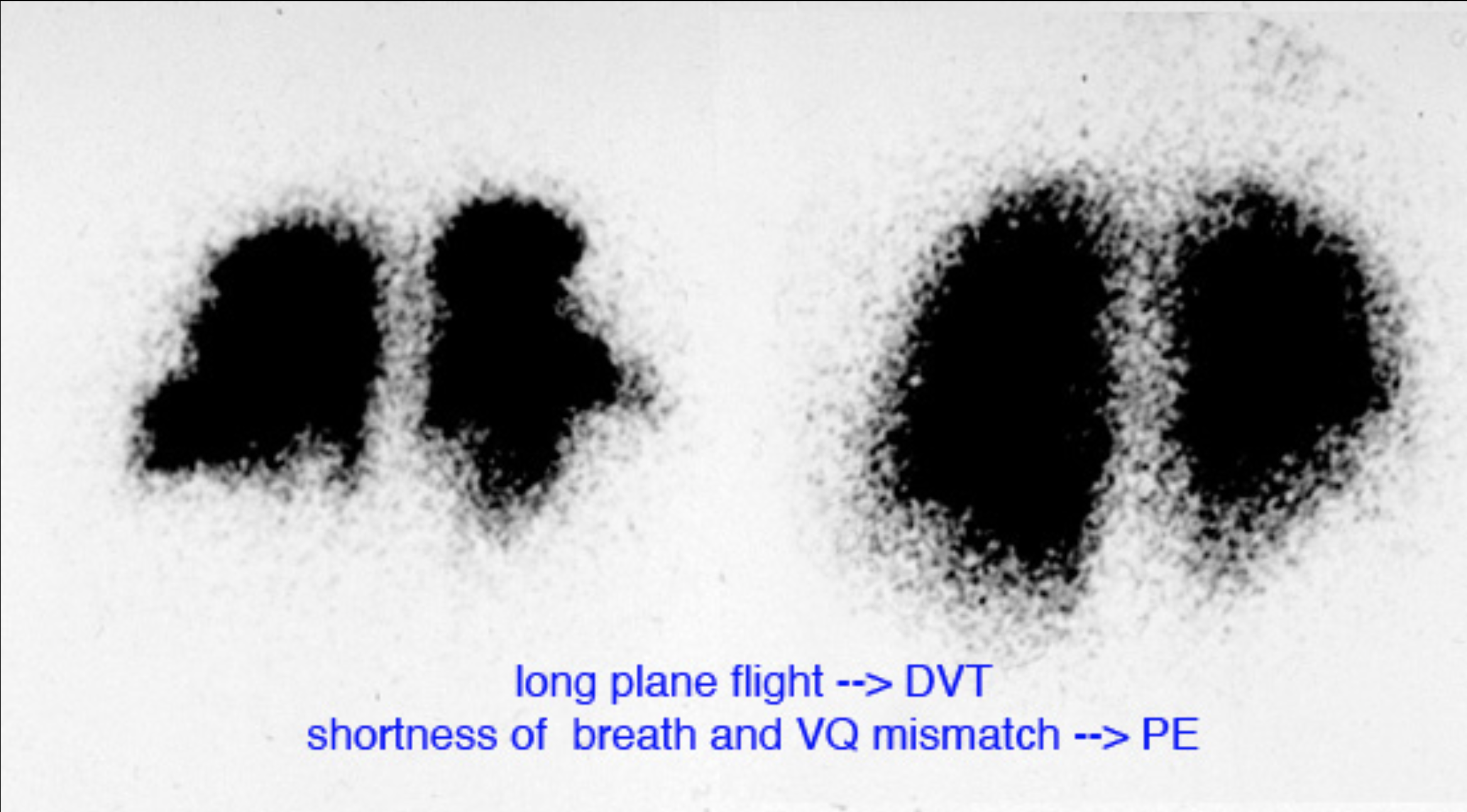
These images show studies that can be done for patients with shortness of breath and risk of pulmonary embolism. For CT scans for this indication, since the focus is on the pulmonary vasculature, intravenous contrast is typically given with timing to optimize contrast in the pulmonary arteries. The mystery study shown below is another way to evaluate a patient for possible pulmonary embolism, and might be done in patients with contraindications to IV contrast for CT (such as renal failure or contrast allergy).
Further Explanation:
Case 3-other imaging
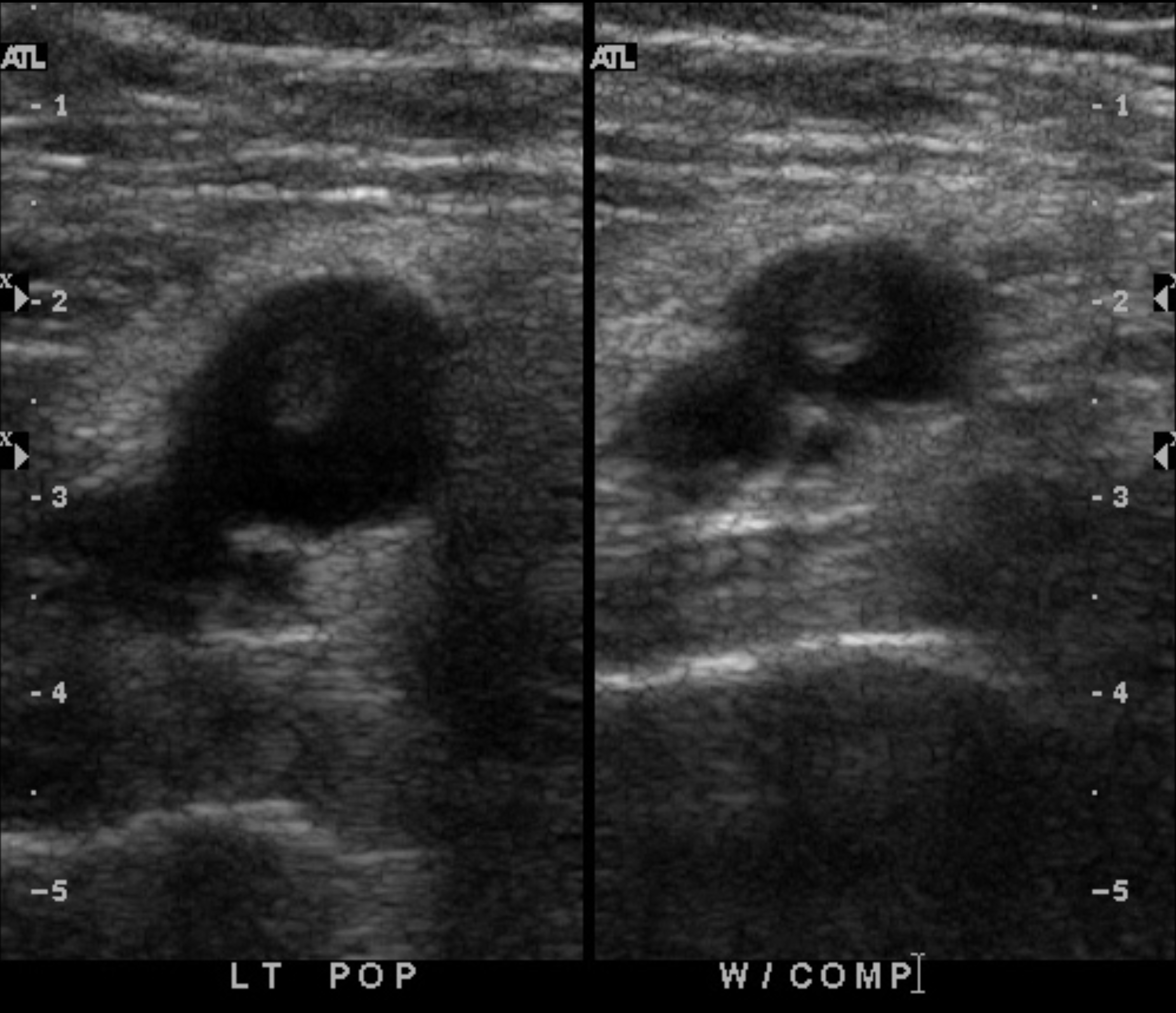
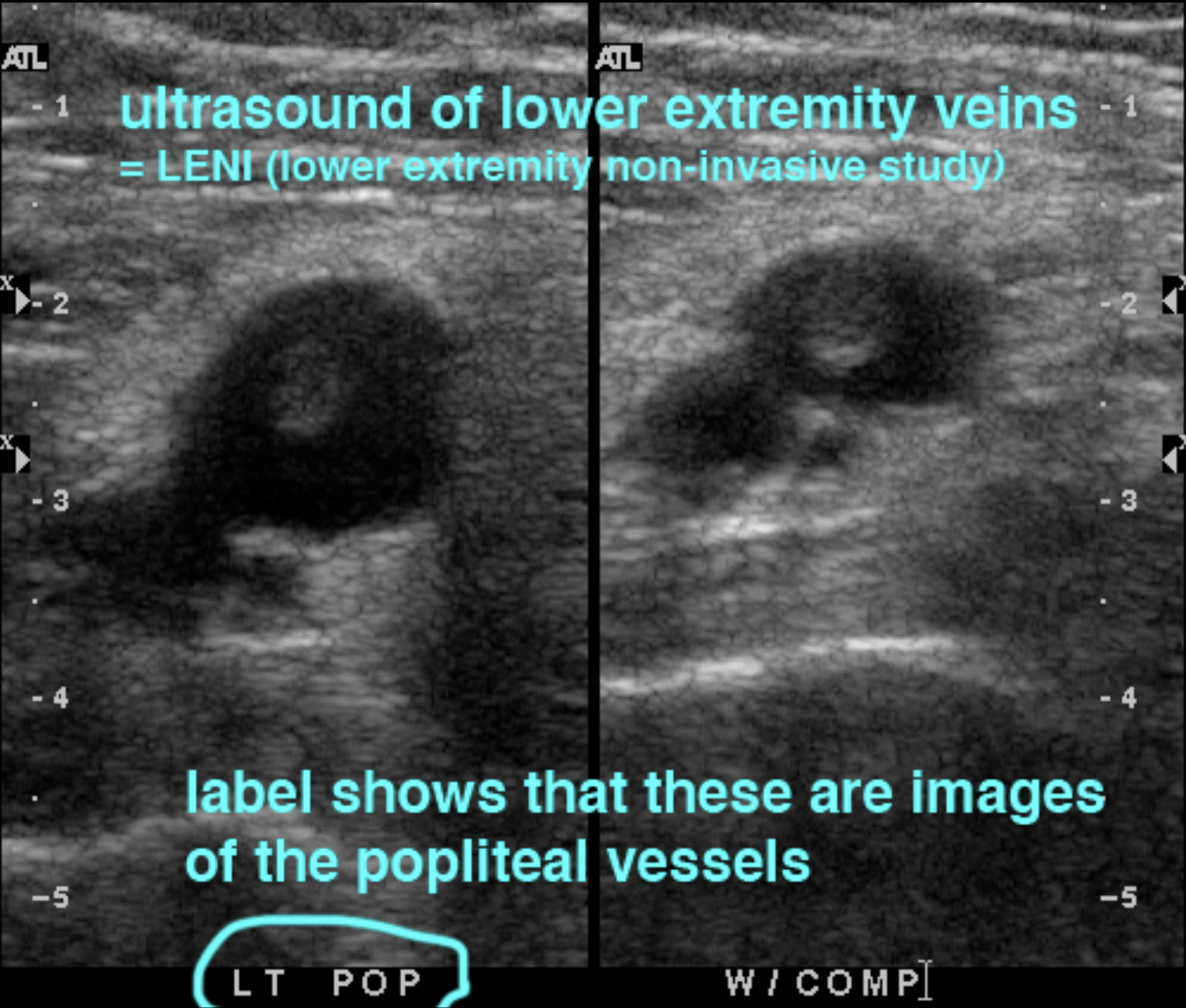
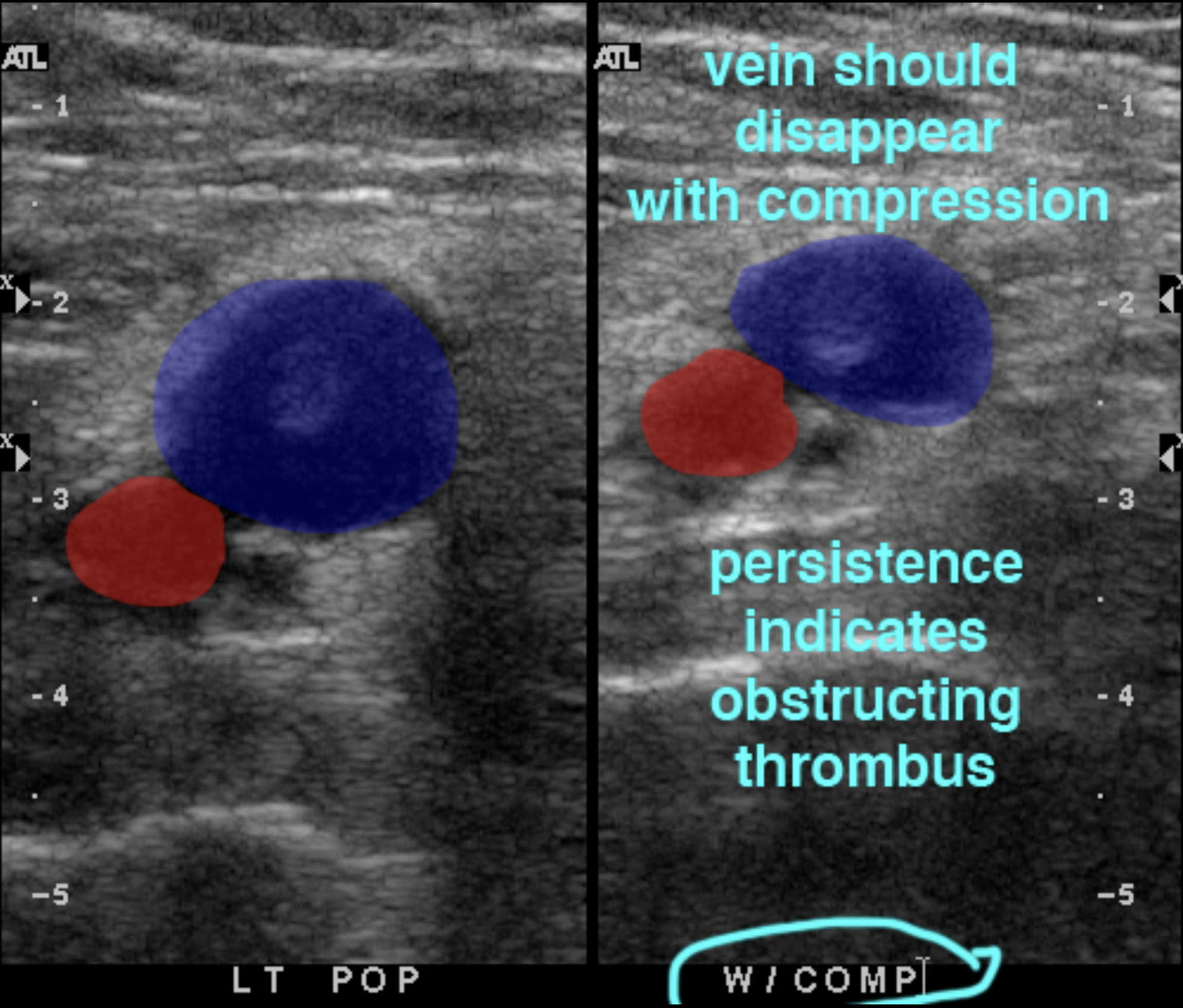
Often, the reason that pulmonary embolism is suspected is because the patient has symptoms of deep venous thrombosis (DVT) in the legs, particularly in a clinical setting consistent with venous stasis (such as long plane flights). This study is done to evaluate the veins of the legs for clot, which may be done in conjunction with a CT for PE (CTPA, or CT pulmonary arteriogram). In fact, if the symptoms and risk status are highly suggestive of PE, a positive study showing clot in leg veins may be sufficient to begin treatment without the need for additional imaging.
Further Explanation:
Case 3-other imaging
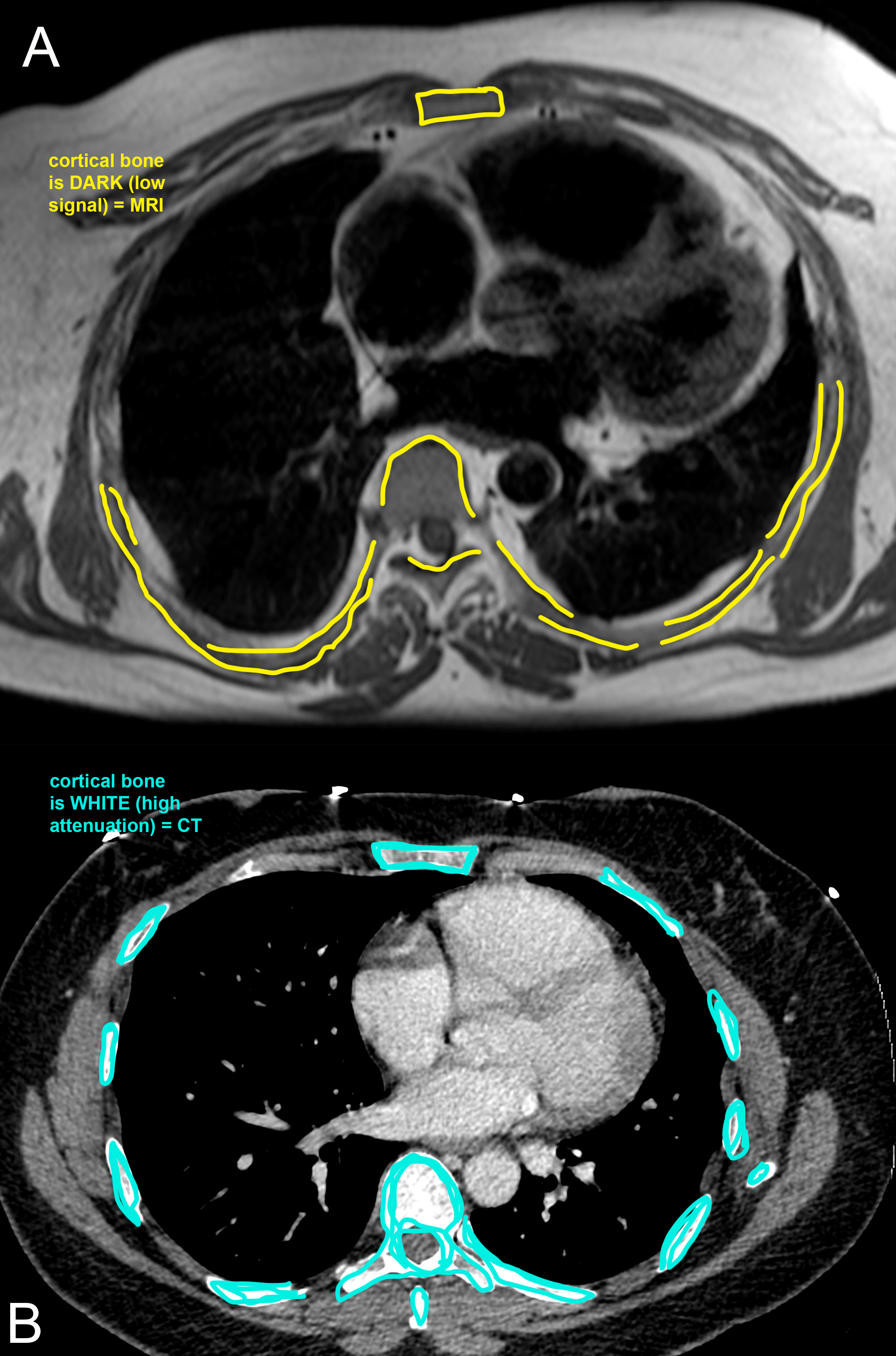
In special situations, MR of the chest may be indicated, but usually not for lung disease. Chest MR does not show the lungs very well, partly because there is motion during the long acquisition, which can take 5-6 minutes per sequence, precluding breath holding. MR is used in the chest more often for pleural, chest wall, mediastinal or cardiac evaluation than for lung disease.
Further Explanation: