Case 2-normal chest CT
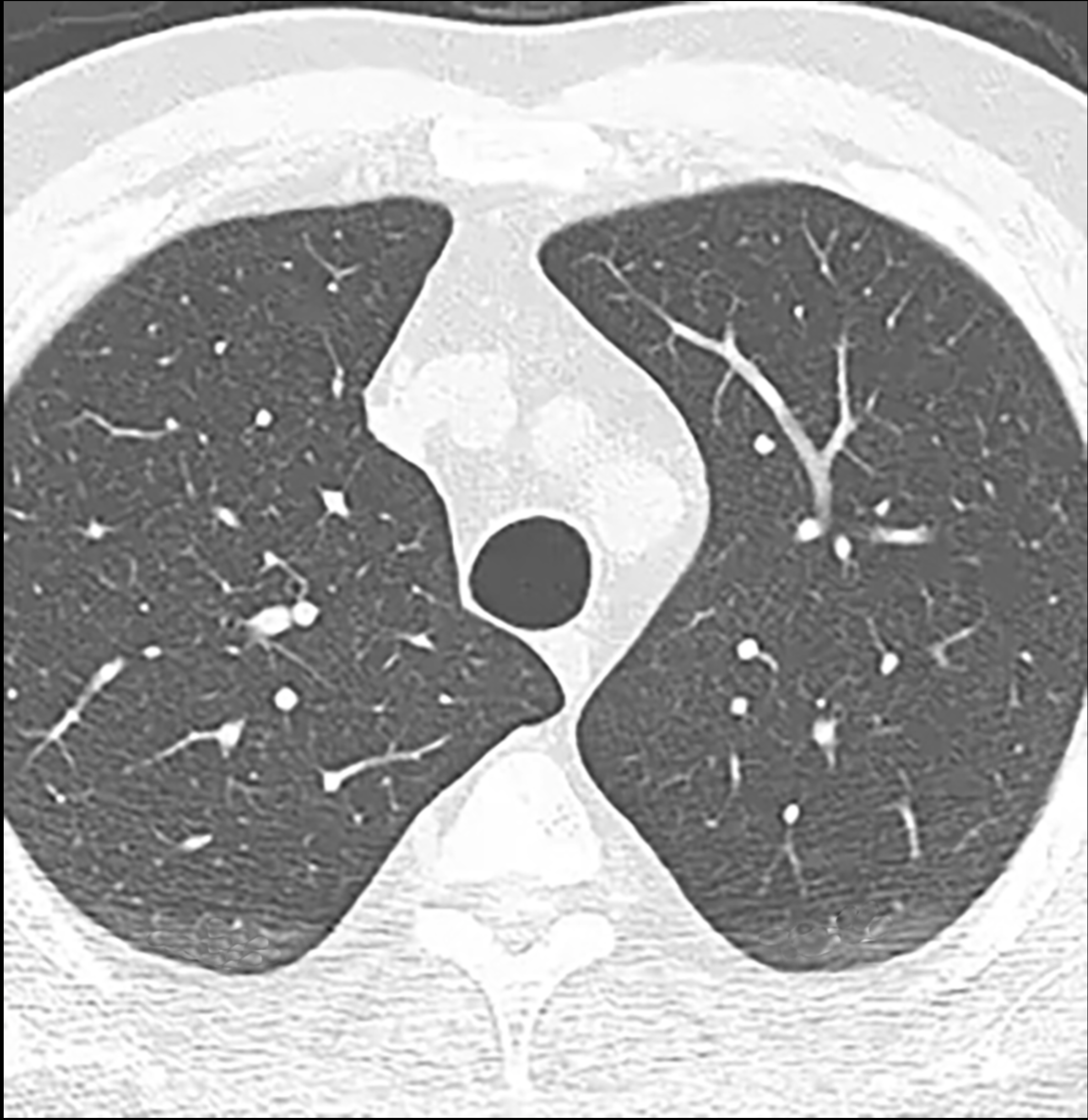
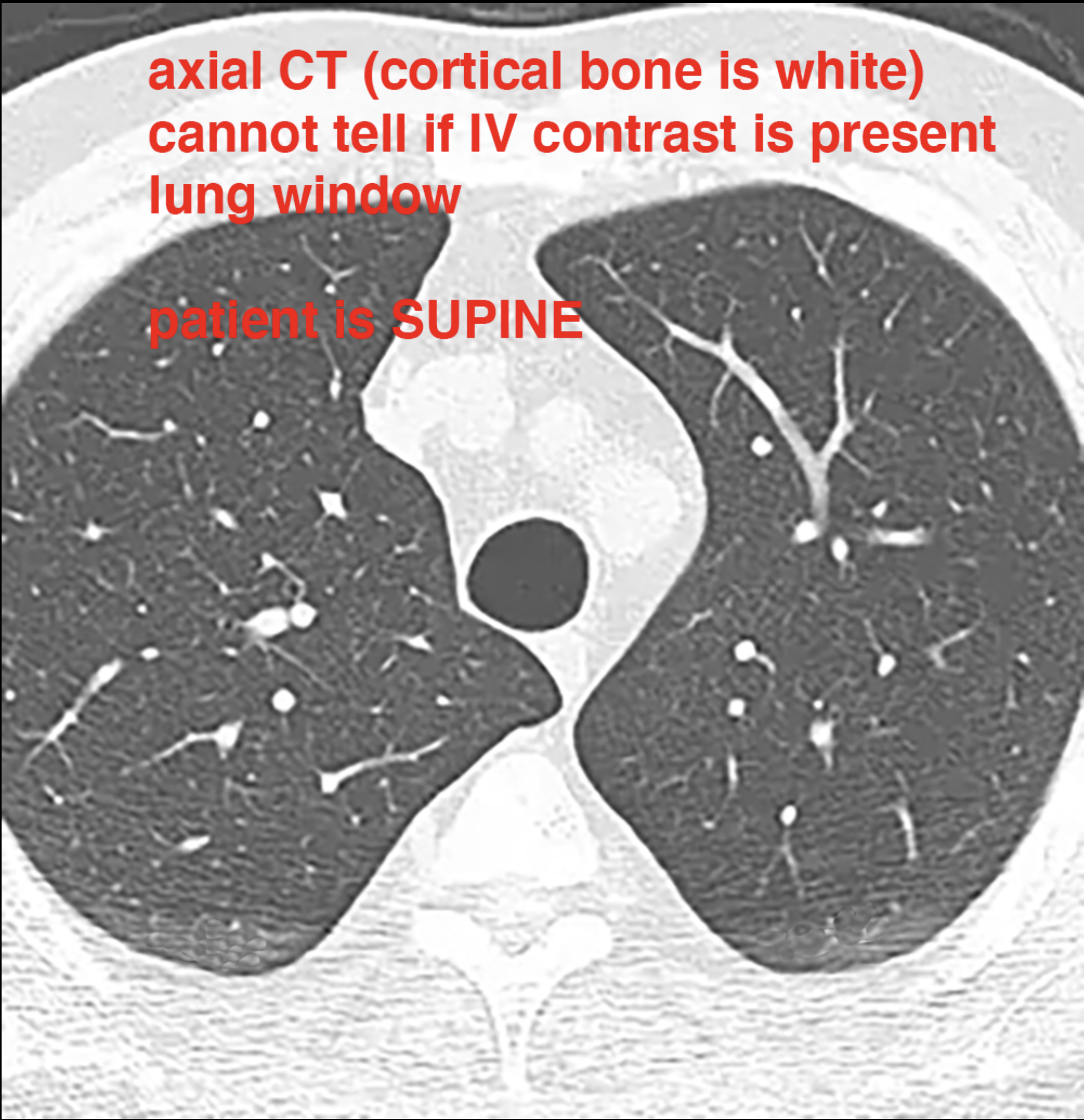
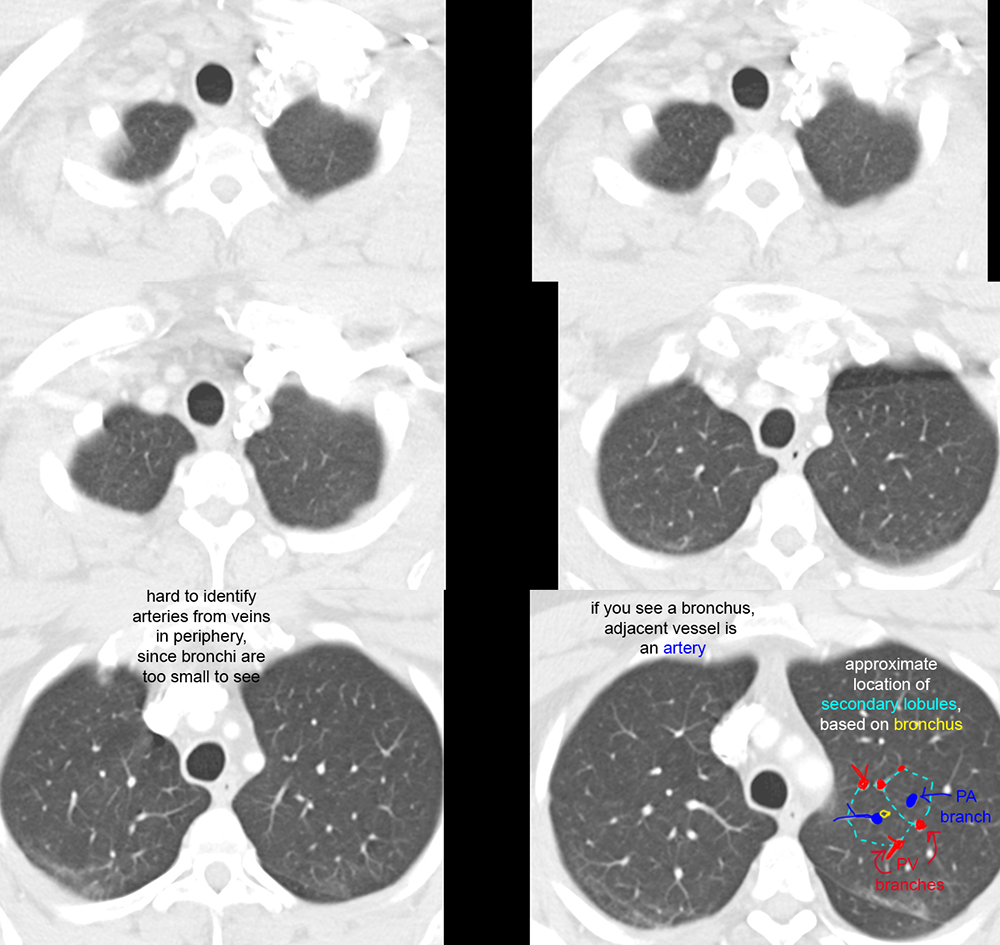
The main problem solving modality for many pulmonary issues, after radiography, is chest CT. The technique for this exam is most often supine positioning, usually with the arms overhead (to lessen artifacts from shoulders overlapping the upper lungs), with the patient holding their breath at maximum inspiration. For imaging the lung itself, intravenous contrast is often not needed.
Further Explanation:
Case 2-normal chest CT
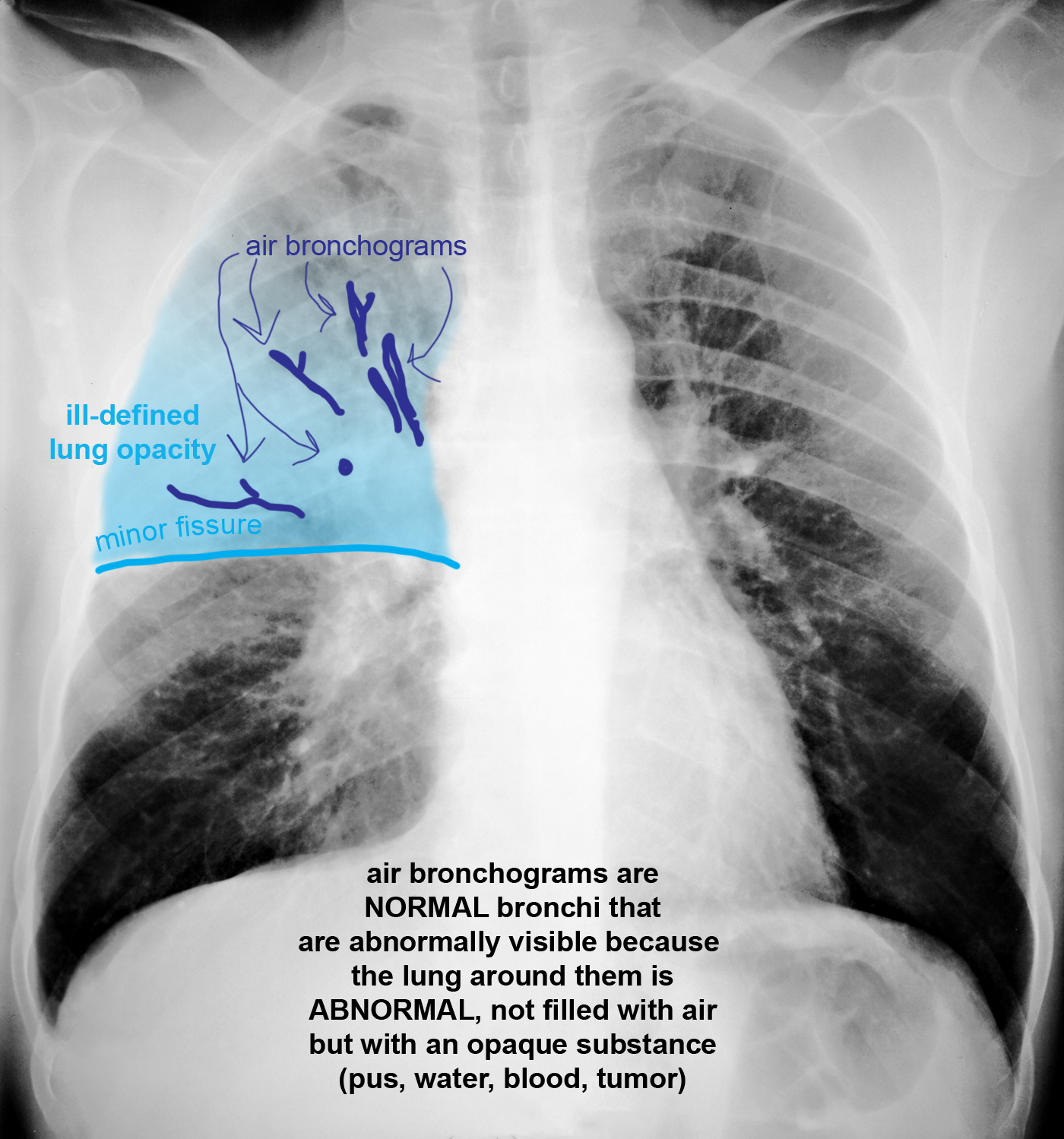
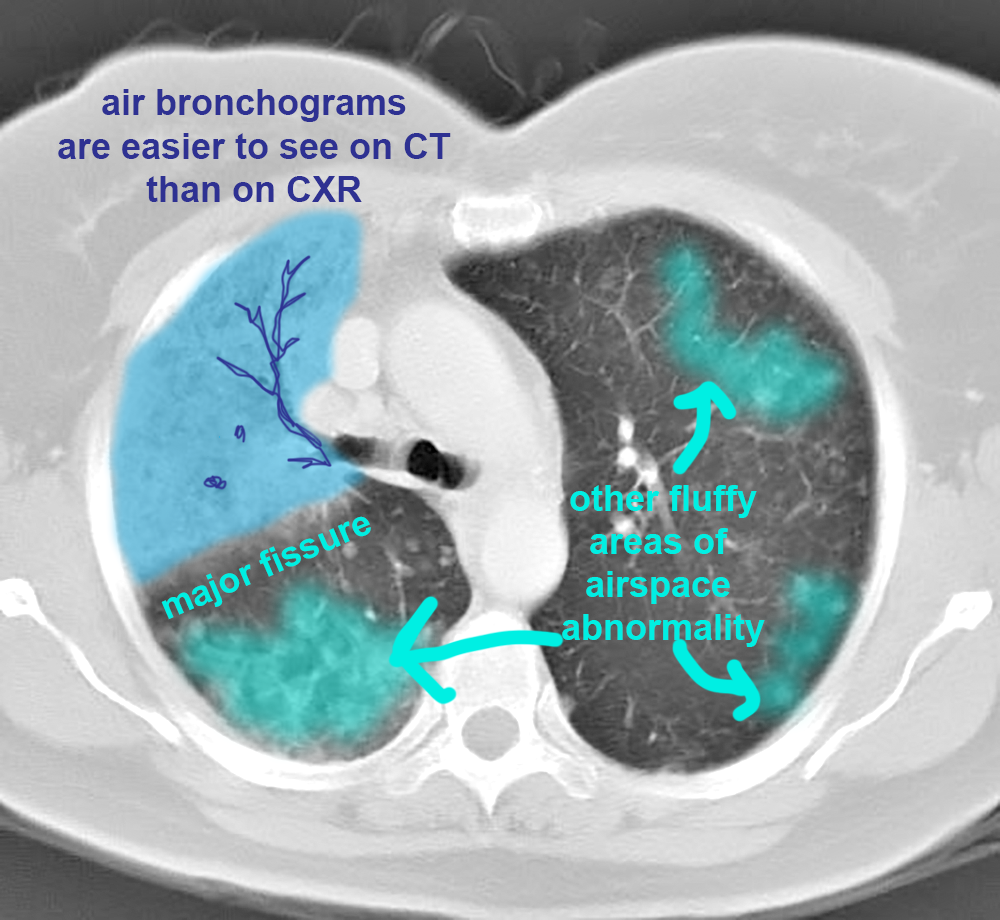
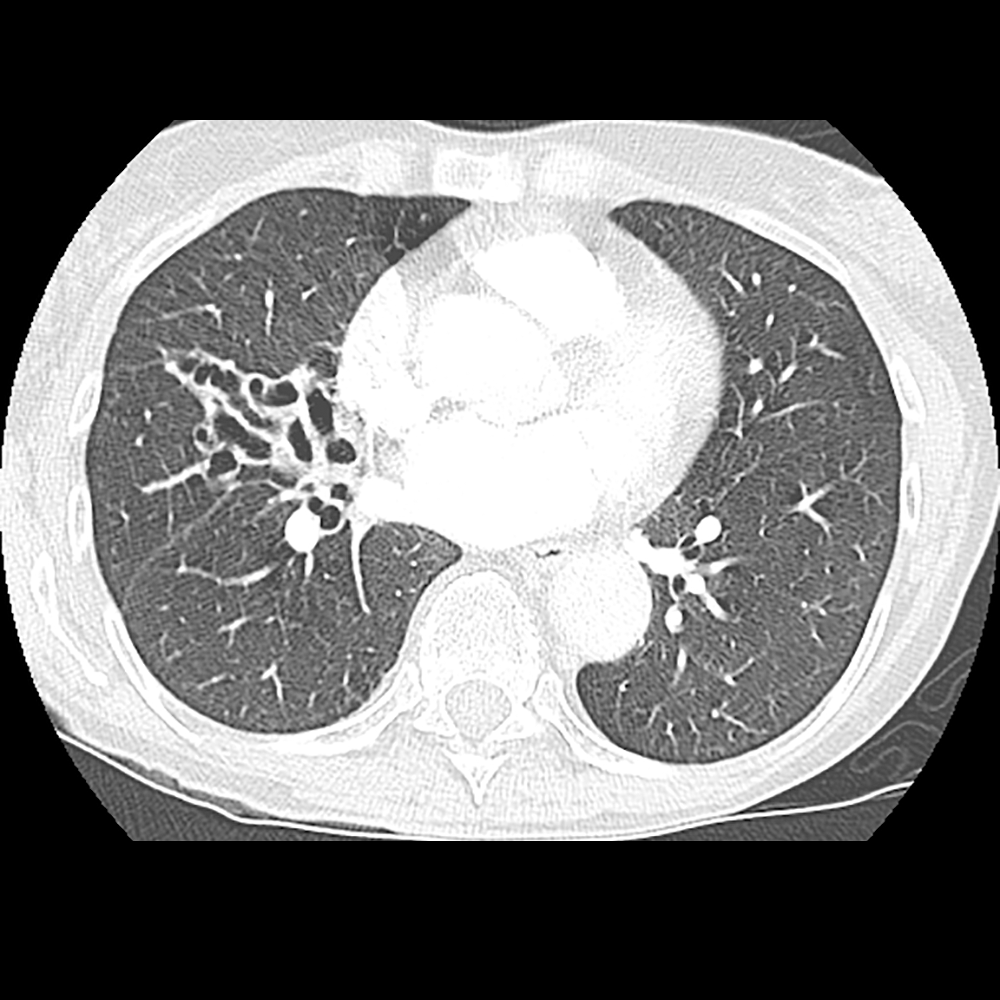
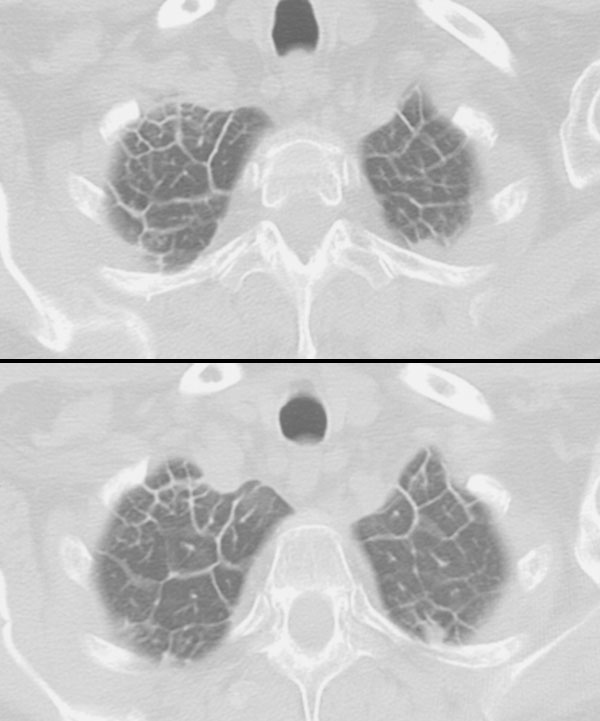
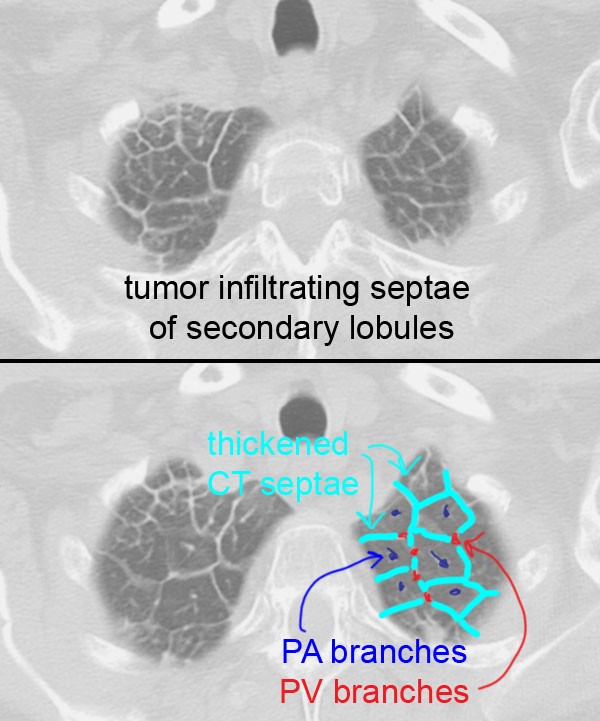
This is a CT in a patient with shortness of breath. A link below shows a CT in a different patient with shortness of breath. Things to think about when you see abnormal markings in the lungs on CT are the DISTRIBUTION of the findings, as well as what descriptive adjectives you would use. Diseases in the interstitium of the lung tend to produce grainy or linear abnormalities on CT, while disease in the airspaces produces hazy, ill-defined abnormalities. And there is often overlap between interstitial and alveolar disease, both on imaging and on pathology.
Further Explanation:

Case 2-normal chest CT
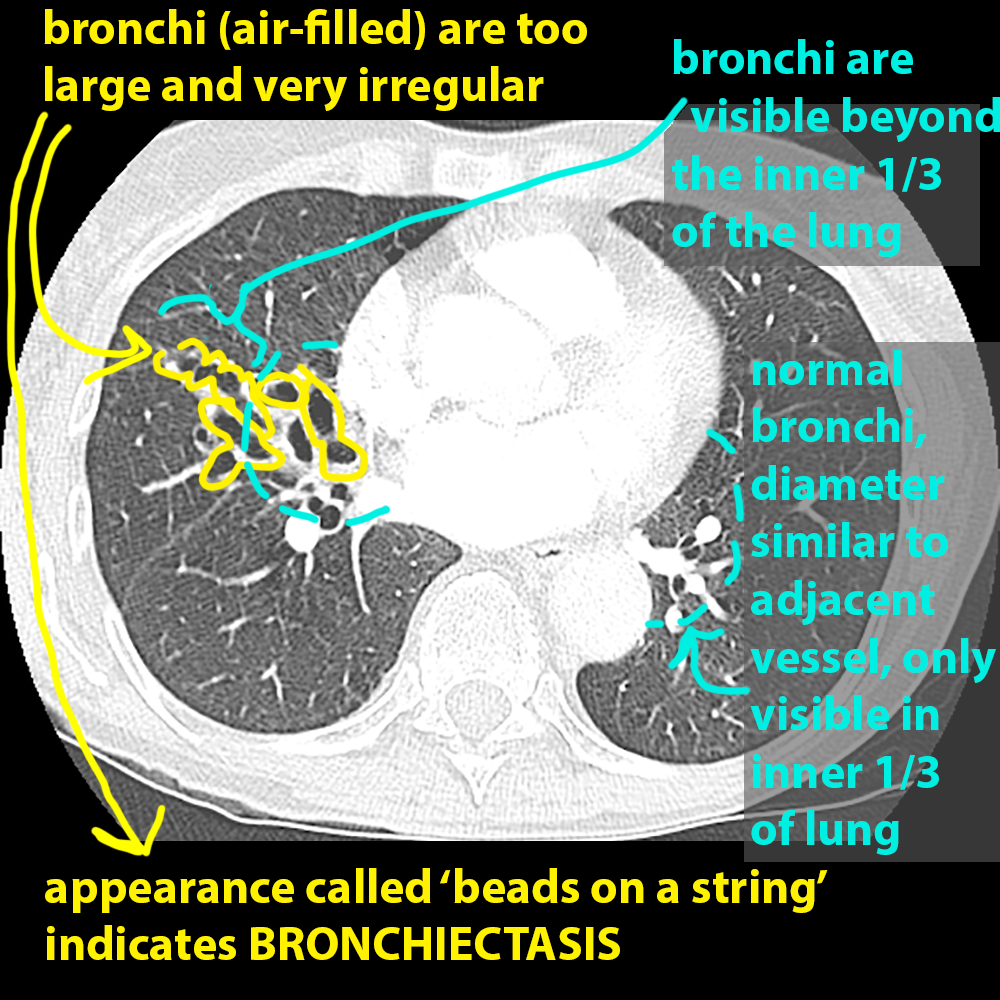
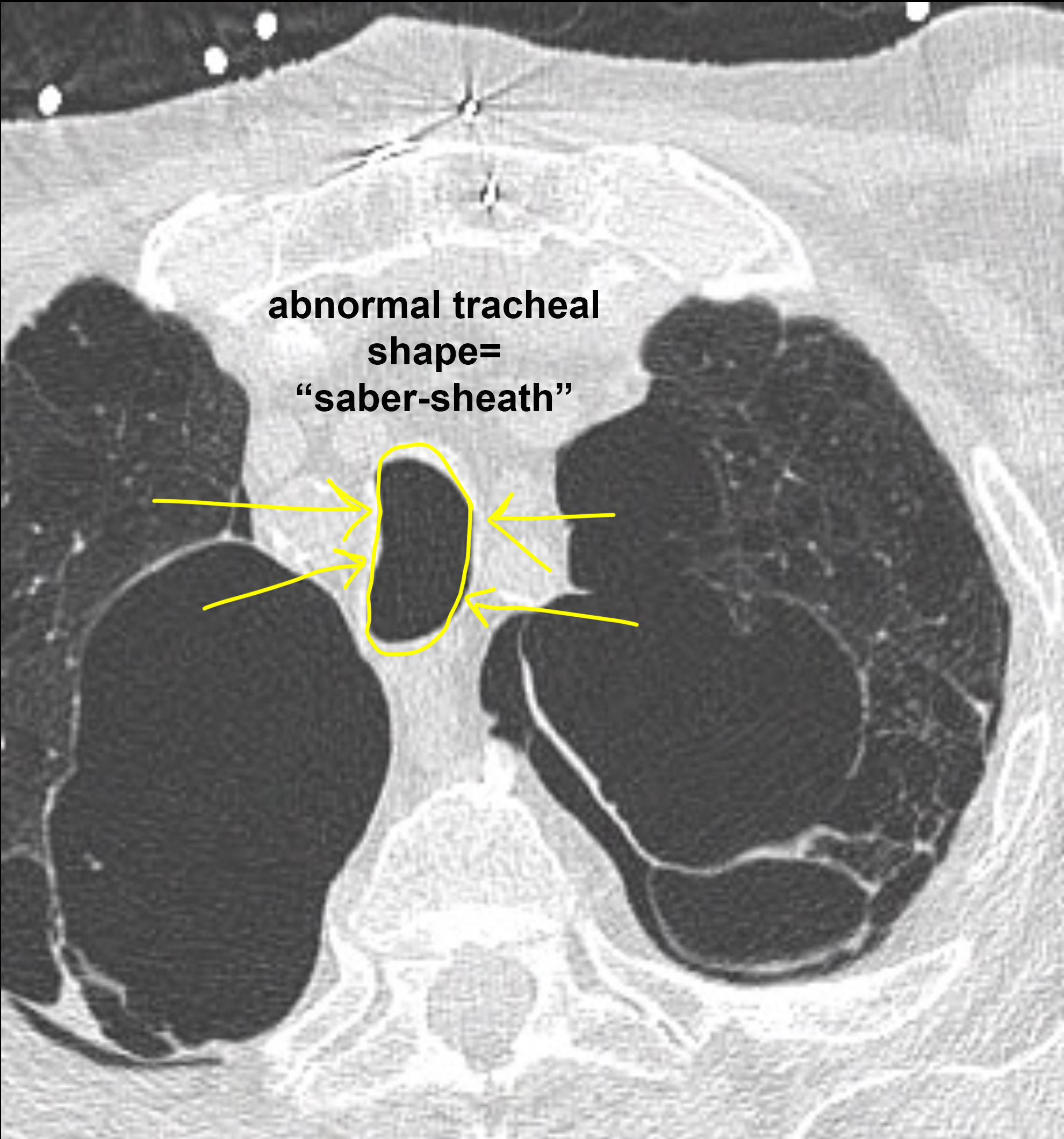
This is a CT of another patient with shortness of breath. What would you imagine the chest radiograph of this patient to look like?
Further Explanation:


Case 2-normal chest CT
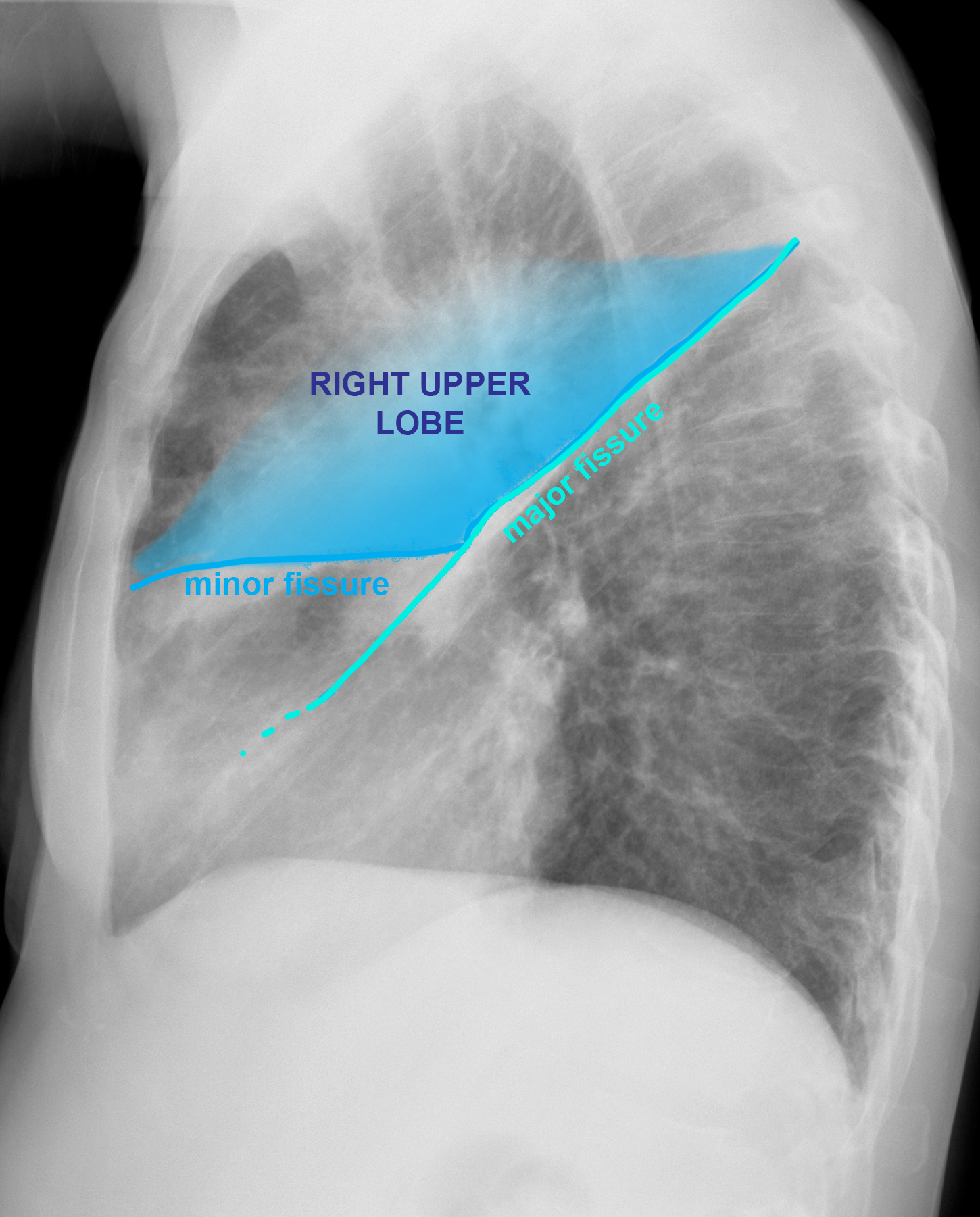
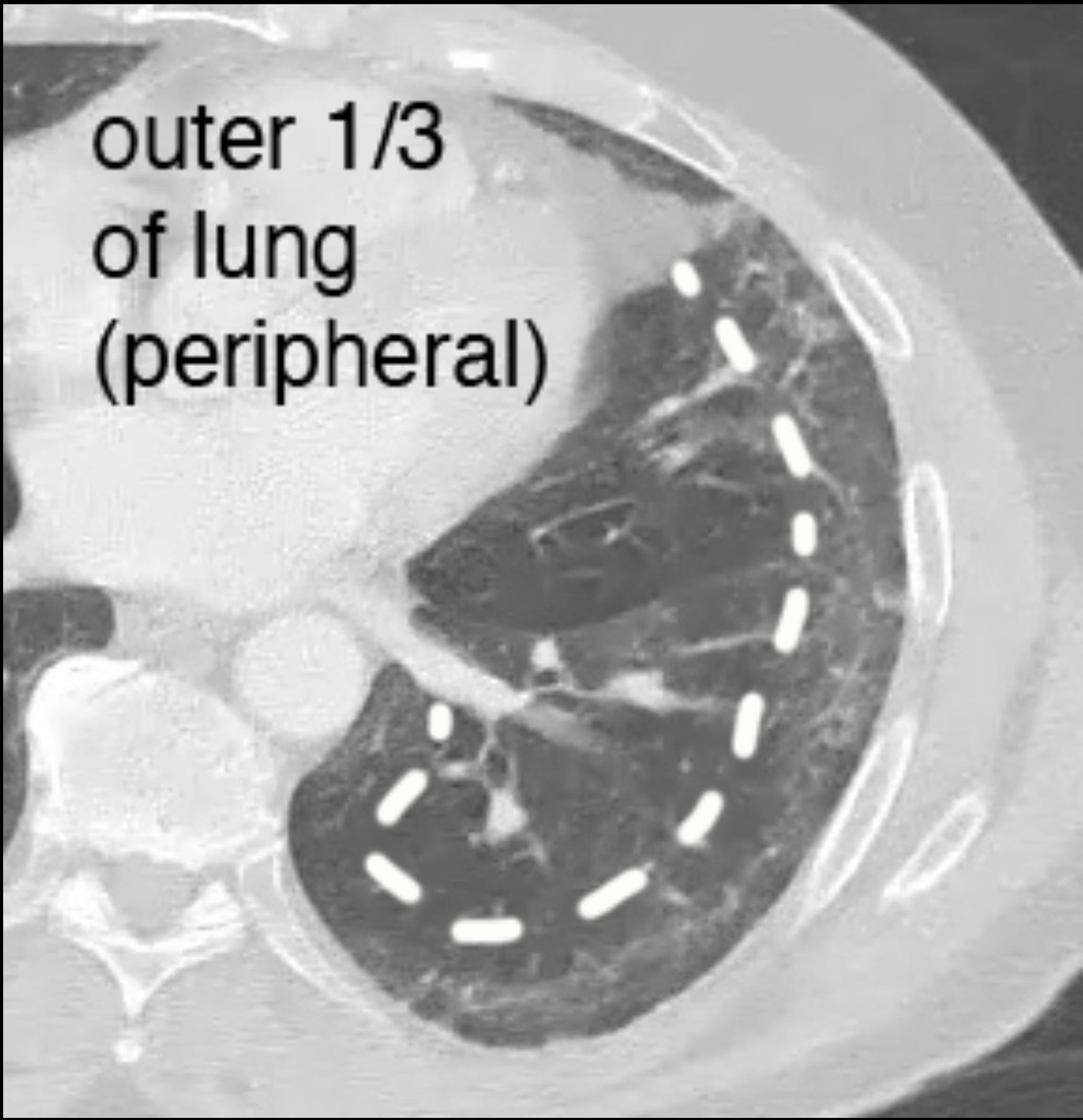
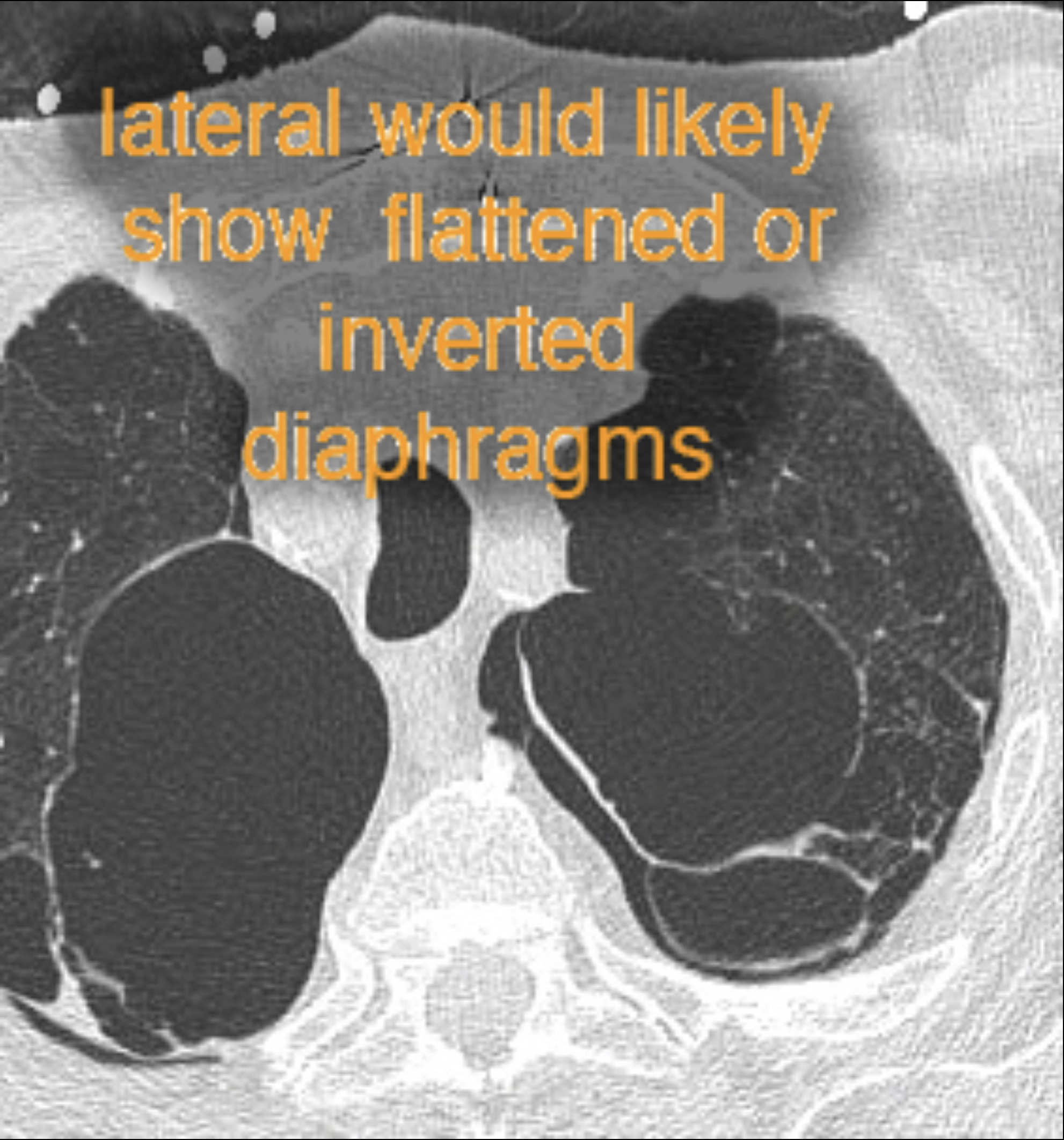
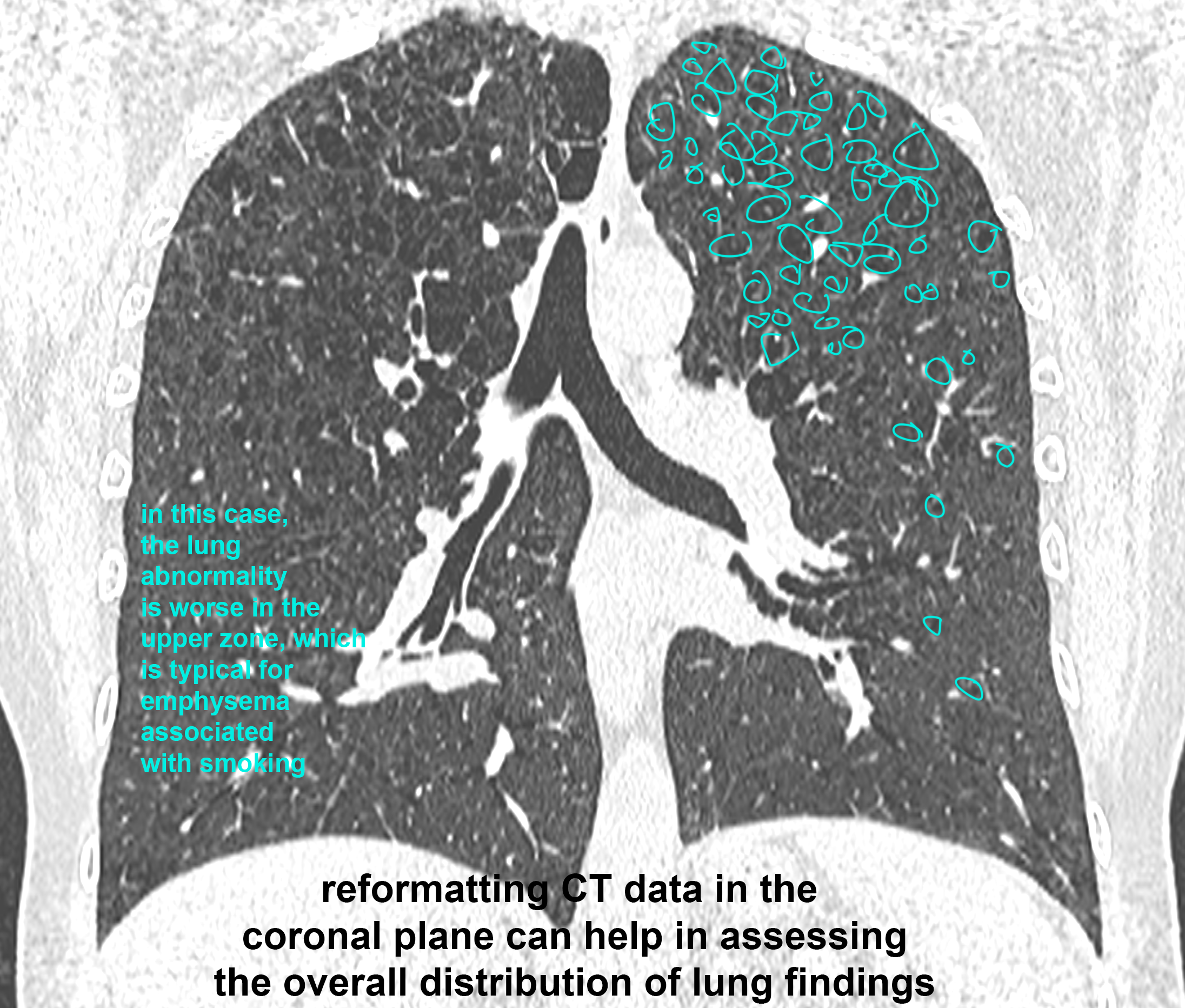
What do you think of this patient's lungs? What other view might be helpful?
Further Explanation: