













Case 4
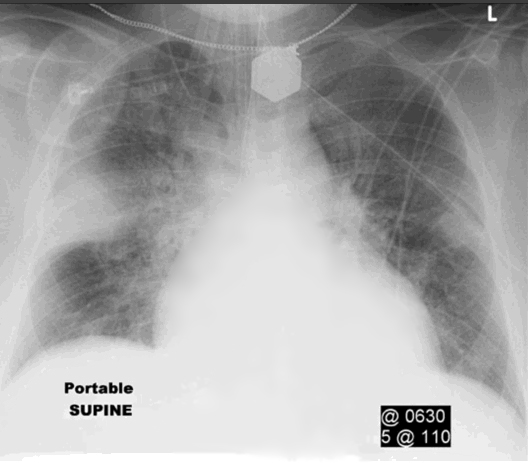
Case 4 concerns the vascular system of the lungs. This 55 year old man had acute chest pain and shortness of breath shortly after getting off a plane from Japan to Boston.
Question 1:
What are pertinent technical parameters of this exam? What descriptive terms would you use for the lung abnormality that is present? What diagnoses would you consider?
×
Answer:
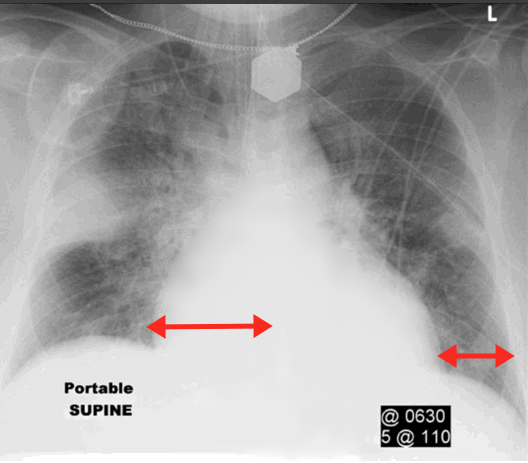
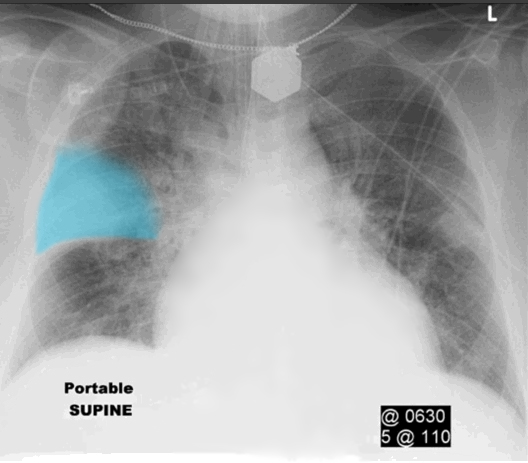
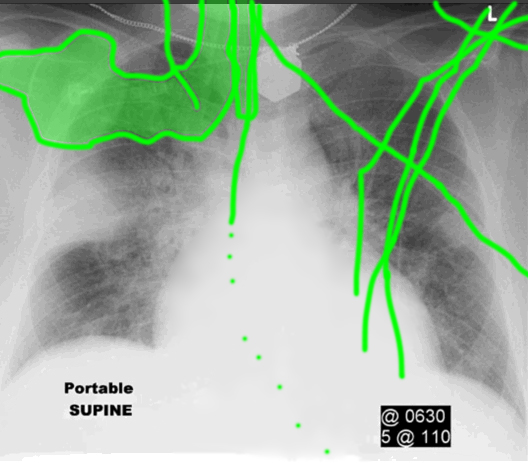
This is a portable chest radiograph in the supine position (see label on image). You could suspect that this might be the case even without the label by noticing all of the support devices that are present. In Session 3, we will go into more detail about many of these devices. There is an abnormal opacity in the right lung with a very smooth and distinct lower edge (the minor fissure) and a hazy upper edge suggesting that it is located in the airspaces and alveoli. This certainly could be another pneumonia, but the history does not mention any fever or cough. The shape and position of the opacity is often termed 'peripheral, wedge-shaped'. The history should suggest another cause for this appearance related to the pulmonary vasculature--pulmonary embolism, with pulmonary infarct. You cannot see an embolism within a vessel on a radiograph, but you might seen the sequelae of blockage of the supply to that section of lung. Note that the heart appears mildly enlarged, although on a portable radiograph it is hard to be sure, as the image of the heart is magnified on an AP projection with short tube-receptor distance, as is typically the case for portable radiographs.
This is a portable chest radiograph in the supine position (see label on image). You could suspect that this might be the case even without the label by noticing all of the support devices that are present. In Session 3, we will go into more detail about many of these devices. There is an abnormal opacity in the right lung with a very smooth and distinct lower edge (the minor fissure) and a hazy upper edge suggesting that it is located in the airspaces and alveoli. This certainly could be another pneumonia, but the history does not mention any fever or cough. The shape and position of the opacity is often termed 'peripheral, wedge-shaped'. The history should suggest another cause for this appearance related to the pulmonary vasculature--pulmonary embolism, with pulmonary infarct. You cannot see an embolism within a vessel on a radiograph, but you might seen the sequelae of blockage of the supply to that section of lung. Note that the heart appears mildly enlarged, although on a portable radiograph it is hard to be sure, as the image of the heart is magnified on an AP projection with short tube-receptor distance, as is typically the case for portable radiographs.
Case 4
This is the next study that was done on a different patient with similar symptoms.
Question 2:
What are pertinent technical parameters for this study? What is the commonest appearance of this condition on chest radiography?
×
Answer:
This is a CTPA--a CT pulmonary angiogram. That means that IV contrast was given and imaging was timed to optimize the amount of contrast in the pulmonary arteries. The study you are shown is in the axial plane, and displayed with mediastinal windows. Because emboli tend to be more frequent in the lower lungs, the images were acquired from bottom to top, instead of the usual order. Most of the time, pulmonary emboli do not produce any abnormality that can be seen on chest radiography. The density on x-ray of clot and flowing blood is the same, so you cannot see a clot in a pulmonary vessel on a radiograph--only on a CT and only with dense contrast present in the pulmonary arteries. So timing of scanning relative to contrast injection is important for visualizing the clot. This patient did not have a peripheral wedge-shaped opacity to suggest a pulmonary infarct. In fact, infarcts in patients with PE are quite rare, as the lung has a rich collateral pathway for blood.
This is a CTPA--a CT pulmonary angiogram. That means that IV contrast was given and imaging was timed to optimize the amount of contrast in the pulmonary arteries. The study you are shown is in the axial plane, and displayed with mediastinal windows. Because emboli tend to be more frequent in the lower lungs, the images were acquired from bottom to top, instead of the usual order. Most of the time, pulmonary emboli do not produce any abnormality that can be seen on chest radiography. The density on x-ray of clot and flowing blood is the same, so you cannot see a clot in a pulmonary vessel on a radiograph--only on a CT and only with dense contrast present in the pulmonary arteries. So timing of scanning relative to contrast injection is important for visualizing the clot. This patient did not have a peripheral wedge-shaped opacity to suggest a pulmonary infarct. In fact, infarcts in patients with PE are quite rare, as the lung has a rich collateral pathway for blood.



