Case 2
This 96 year old male became confused and somnolent after a fall in a nursing home.
Question 1:
a) What is this study?
This is an axial head CT without IV contrast.
b) Why are there dark streaks running through some of the images?
The dark streaks on the lowest images are due to metal related to dental work. The CT reconstruction algorithm has problems reconstructing images when there are very dense things in the slice. Several of the images higher in the head also have a different artifact that represents motion of the patient during image acquisition.
Case 2
Here are two selected images from the prior CT sequence.
Question 2:
a) Why was no IV contrast given in this setting?
In the setting of trauma, acute hemorrhage is a clinical consideration. For head CT scanning in this situation, no IV contrast should be given, so that any abnormal white areas will either represent calcifications or hemorrhage.
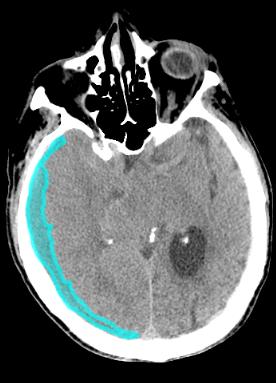
b) Do you see any dense material that might represent acute hemorrhage?
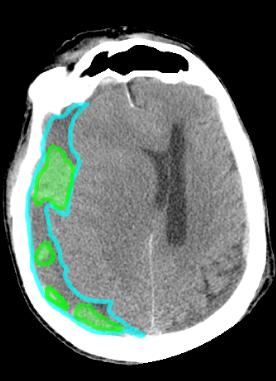
Yes there are several areas of high attenuation along the right side of this scan. They are best seen on slice 2 below.


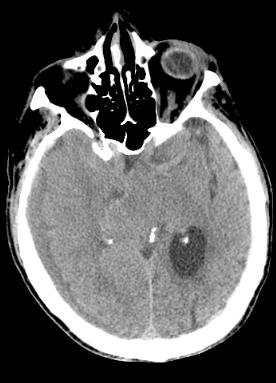
Case 2
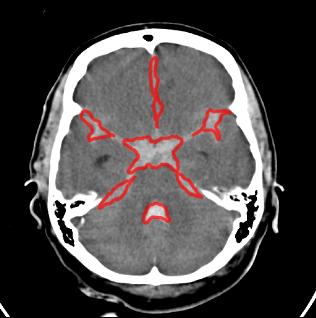
This is one of the images from this patient's head CT. Try to identify the structures labeled below.
Question 3:
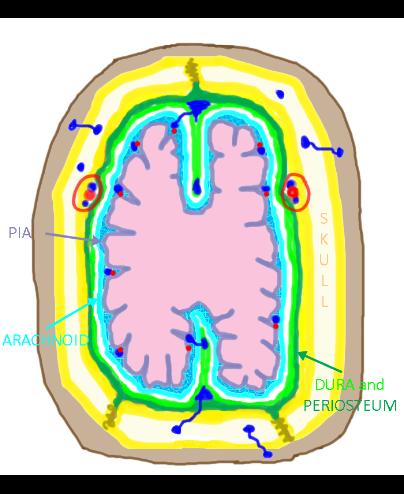
a) Where are calcifications 1 and 2? Are they abnormal?
Calcifications 1 lie in the lateral ventricles bilaterally (outlined in yellow). This is a common place for normal calcification of the choroid plexus. However it is not normal for the two lateral ventricles to be so different in size. Calcifications 2 are in the region of the pineal gland, another common place for normal calcifications. However they are not midline in position, as the pineal gland should be.
b) What is structure 3?
The structures outlined in red are the middle cerebral arteries and basilar artery, seen only on the left and displaced from their normal position.
c) What are the two 'abnormalities' outlined on the original CT and on slice 2?
There is a crescent-shaped collection with mixed high and low attenuation wrapping around the right side of the head and displacing the brain tissues. This appearance is consistent with a hemorrhage consisting of fresh and older blood. The older blood is lower in attenuation, as the cellular parts have separated out, leaving fluid density serum behind. This suggests that bleeding has been intermittent.
d) What is the significance of the midline position?
There is considerable shift of the midline of the brain to the left, indicating increased pressure within the cranium. This can compress vital structures in the brainstem, including the vascular structures of the circle of Willis, and lead to serious neurologic complications.






Case 2
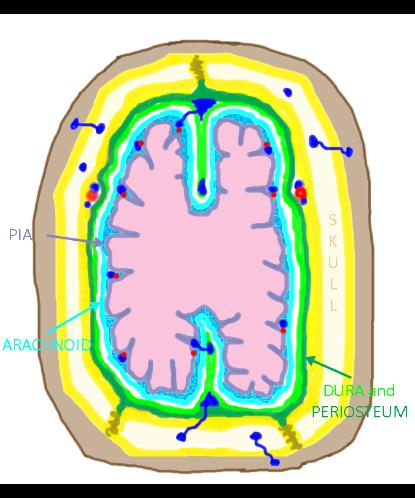
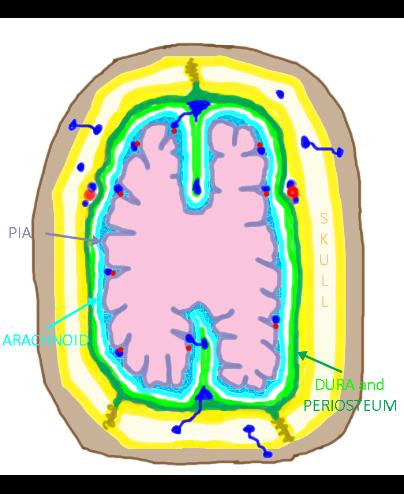
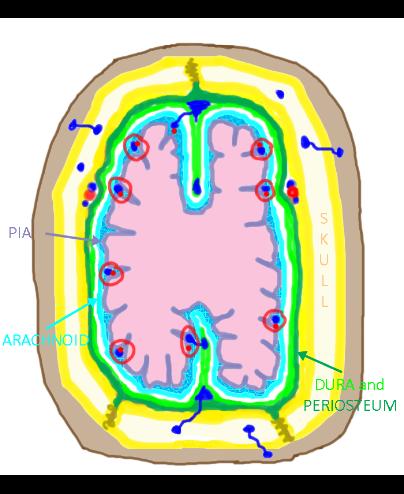
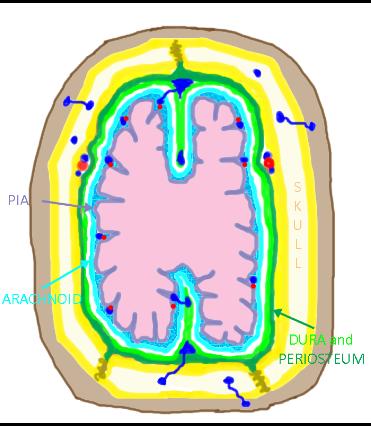
This is a cross-sectional diagram corresponding to an upper head CT section plane. Skin and subcutaneous fat are shown in brown. The inner and outer tables of the skull are shown in yellow. The marrow space of the skull is shown in white. The brain is shown in pink.
Question 4:
a) What colors indicate the location of dura, arachnoid and pia on this diagram?
The dura is the thin light green line, inseparable from the dark green line that represents the periosteum of the inner table of the skull. The arachnoid is shown in light blue. The pia mater extends down into each sulcus on the surface of the brain and is shown in purple.
b) What vessels are indicated by labels 1, 2, 3 and 4 below?
Vessels 1 are middle meningeal arteries and veins, running just on the inside of the skull and producing grooves on the inner surface of the skull. Vessels 2 are dural venous sinuses. Those in the outer part of the diagram are two cross-sections of the superior sagittal sinus and those more central in location are two cross-sections of the inferior sagittal sinus. Vessels 3 are cerebral vessels, distal branches of the circle of Willis. Vessels 4 are bridging veins that connect the surface cerebral veins to the dural sinuses.
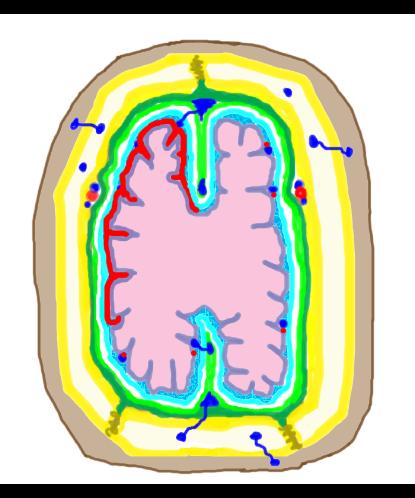
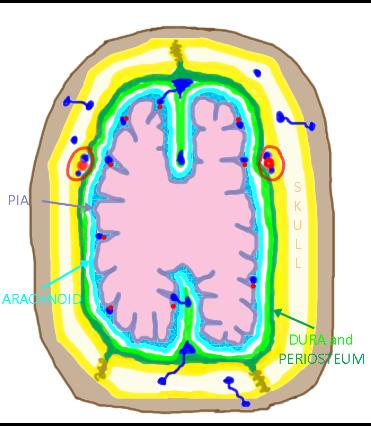
c) Which vascular structures were likely involved in this patient's injury?
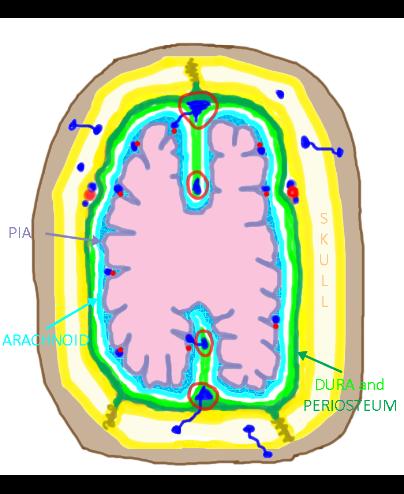
The 'abnormality' label below shows a crescent-shaped hemorrhage as was seen in our patient. This is a common injury in elderly patients after a fall. The deceleration of the brain within the skull can tear the bridging veins and lead to rapid accumulation of blood in the subdural space (between dura and arachnoid). This yields a characteristic crescent-shaped collection.
Case 2
This 25 year old male was involved in an altercation and suffered head trauma. He is was agitated and vomiting but is now becoming somnolent.
Question 5:
a) What is this study?
This is an axial noncontrast head CT scan.
b) Do you see any soft tissue abnormalities outside of the brain that may indicate the site of trauma?
There is soft tissue swelling in the right temporal region.
c) Do you see any high attenuation intracranially that might represent acute hemorrhage?
Yes, there is a high attenuation collection on the right just deep to the inner table of the skull.
Case 2
This is a selected image from the previous CT series, with labels indicating the findings.
Question 6:
a) How would you describe the shape of the intracranial hemorrhage?
It is outlined in red below, and is lens-shaped. This is different from the previous case, where the blood was in a crescent shape.
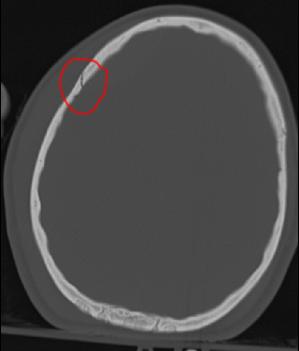
b) Given the history of trauma, what is shown on slice 2 (below) that was not evident on the initial brain window images?
Slice 2 is a bone window at the same level as the initial image. This shows a non-displaced skull fracture.

Case 2
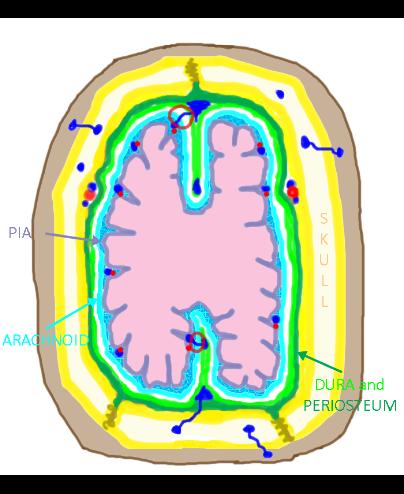
This is the diagram of the layers of the skull, meninges and brain.
Question 7:
a) What vessels would be most likely to be injured by a skull fracture, as this patient suffered?
The middle meningeal artery and its branches run immediately inside the inner table of the skull (see label below), and are vulnerable to injury by skull fractures.
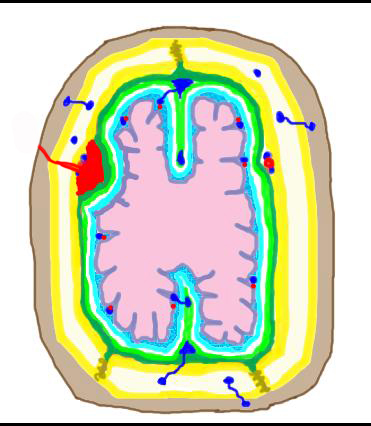
b) What term is applied to blood that collects in this case, shown below by the 'abnormality' label?
Blood that collects in the potential space between the dura and inner table periosteum is called an epidural hematoma. Because the periosteum and dura are tightly adherent, more force is needed for blood to collect in this space than for a subdural hematoma, but as this is often arterial bleeding, it is under enough pressure to peel the dura off the periosteum.
Case 2
This is a 58 year old female with the sudden onset of the worst headache of her life.
Question 8:
a) What kind of study is this?
This is a noncontrast axial head CT scan.
b) How would you describe the abnormal high attenuation on these images?
On these images, the high attenuation material surrounds the brain and extends in finger-shaped projections down into each sulcus.
Case 2
This is a selected image from our patient's noncontrast CT scan. Red outlines the areas of hemorrhage, which are high attenuation relative to brain parenchyma.
Question 9:
a) Where is this blood located?
This is an example of subarachnoid hemorrhage, which typically extends into the sulci of the brain giving a finger-like appearance.
b) In addition to the blood overlying the brain surface, where else is blood seen on these two images?
There is blood in the third ventricle, in the 4th ventricle, and in the lateral ventricles. The amount of intraventricular hemorrhage is correlated with outcomes in subarachnoid hemorrhage. Outcomes are poorer for patient with more intraventricular blood.

Case 2
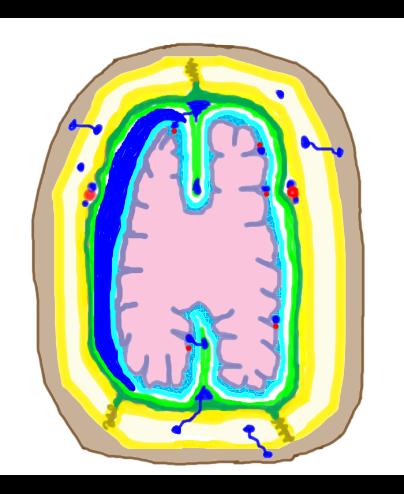
This is the diagram of skull, meninges and brain again.
Question 10:
What vessels are the likeliest origin of bleeding into this space?
Subarachnoid hemorrhage usually arises due to bleeding from cerebral vessels, either arteries or veins. Bleeding from the circle of Willis is arterial and most often due to a ruptured aneurysm, which was the cause in this case. Bleeding from peripheral branches may be arterial or venous, related to trauma or tumor. Hemorrhage from a brain tumor can enter the subarachnoid space or ventricles or both depending on the location of the tumor.