Case 2
This is an image of a 51 year old man with chronic left shoulder pain and history of past left shoulder dislocation.
Question 1:
a) What is this image?
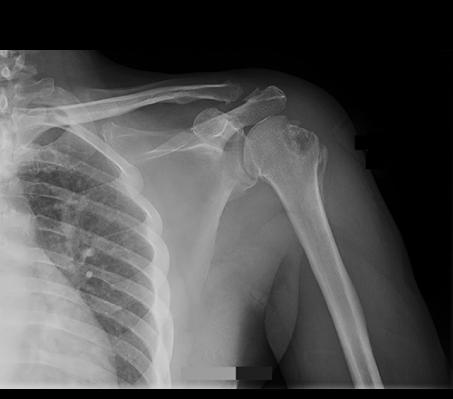
This is an AP radiograph of the shoulder with the humerus in external rotation.
b) Does the humerus appear normal?
No, the humeral head is deformed with a dent out of the lateral margin. Click on the normal comparison link to see the normal shape of the humeral head.
c) Do you think that an AP and lateral view are adequate for imaging the shoulder?
No, the shoulder is a very complex shape (unlike the forearm or femur or other long bones), and many different projections are typically performed to get an adequate view of this region. A true lateral view, in particular. is not very useful as there is too much overlap of the opposite shoulder on the image. Other specialized views are needed to see all of the bony components of the shoulder.
Case 2
This is the same AP view of the shoulder shown previously. Try to identify the bony landmarks before clicking the labels below.
Question 2:
a) Since a true lateral view of the shoulder is not a very useful image due to overlap, how can we get orthogonal views of the humeral head?
Orthogonal views (views at 90 degrees from each other) are routinely done in bony radiography. For a simple long bone like the radius or the tibia, an AP and a lateral view can be sufficient. For a complicated region like the shoulder, special views are needed. To get two orthogonal views of the humeral head, we can do two AP views, one with internal rotation and one with external rotation of the humerus. This gives us two views of the humeral head at about 90 degrees from each other. This does not solve the problem of orthogonal views of the other bones of the shoulder (scapula, clavicle), but it does allow us to better evaluate the proximal humerus.
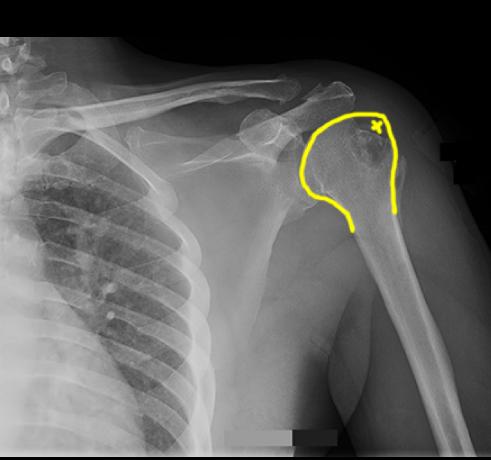
b) What specific part of the humeral head is missing (indicated by the 'x' on the labeled image of the humeral head below)?
Since the humerus is in external rotation, this brings the greater tubercle into a lateral position. So the greater tubercle is missing at the spot marked with an 'x'.
c) How does the appearance of the humeral head relate to the patient's prior history of shoulder dislocation?
When the shoulder dislocates, the head of the humerus can sometimes impact on the inferior portion of the glenoid, leading to a crushing injury in the region of the greater tubercle, called a compression fracture. This specific fracture is given a special name--Hill Sachs deformity. It indicates prior shoulder dislocation.

Case 2
This is the previous normal comparison image for you to practice identifying normal bony landmarks.
Question 3:
a) What attaches to the coracoid process?
The coracoid process of the scapula provides attachment for three muscles: short head of the biceps brachii, coracobrachialis, and pectoralis minor.
b) What attaches to the greater tubercle of the humerus?
Three of the rotator cuff muscles attach to the greater tubercle (tuberosity): supraspinatus, infraspinatus, and teres minor.
c) What attaches to the lesser tubercle of the humerus?
Subscapularis muscle attaches to the lesser tubercle (tuberosity).

Case 2
This is the normal shoulder radiograph, AP view in external rotation, with structures for you to identify.
Question 4:
a) What are the structures indicated below?
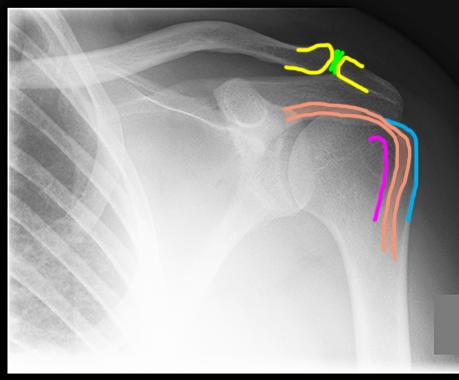
The distal clavicle and acromion are shown in yellow, forming the AC joint, with the region of the joint space and articular cartilage indicated in green. The greater tubercle (tuberosity) of the humerus is shown in blue and the lesser tubercle (tuberosity) in purple. The long head of the biceps in the intertubercular groove is shown in orange.
b) Where does the long head of the biceps attach?
The long head of the biceps passes up in the intertubercular groove, then arches over the humeral head to reach the superior part of the glenoid and inserts at the supraglenoid tubercle the scapula.
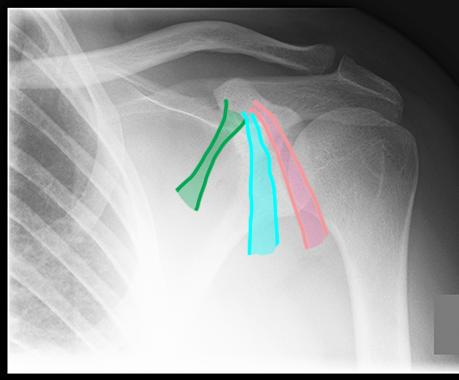
c) What are the three tendons shown below, attaching to the coracoid process?
The most medial tendon (shown in green) is pectoralis minor, the next more lateral tendon (shown in blue) is coracobrachialis, and the most lateral tendon (showing pink) is the short head of biceps brachii.

Case 2
These images are from other patients.
Question 5:
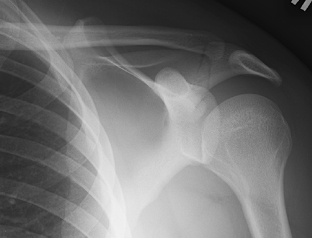
a) What is the difference between the first image and the 'other view', shown below?
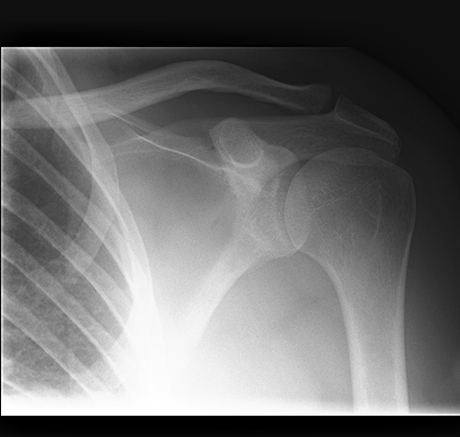
The first image is an AP radiograph in external rotation. The other view is an AP radiograph in internal rotation. In external rotation, the greater tubercle sticks out laterally. In internal rotation, the lesser tubercle sticks out medially. Try to identify these structures on these two images.
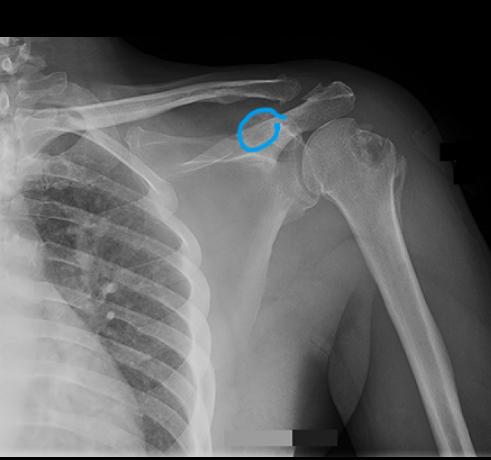
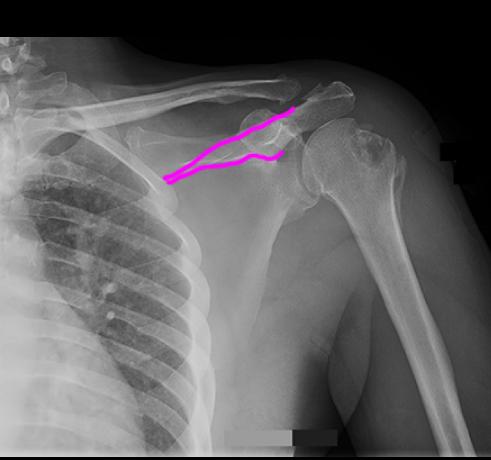
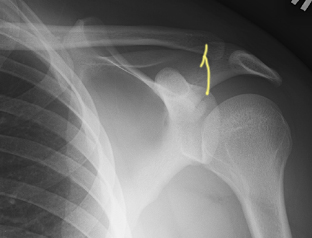
b) There is a non displaced fracture shown on this image (click below to see labels). What bone is involved with this fracture?
This fracture goes through the scapula, in the region of the base of the acromion process. This is not a common site for fracture and may have been due to a direct blow to the area. To better delineate the fracture, a CT is probably needed, since it involves a complex bone that is hard to completely image with radiography.

Case 2
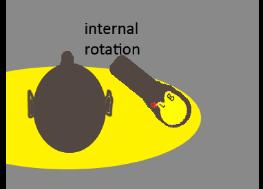
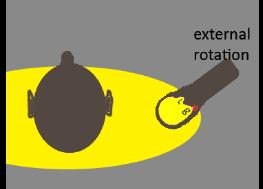
These diagrams show the relative positions of the greater and lesser tubercles on the humeral head, with the arm in neutral, internal rotation and external rotation positions. Radiographs are also shown with the two tubercles outlined. In the diagrams, assume that the elbow is flexed 90 degrees, and that the distal part of the limb in the diagrams represents the position of the forearm.
Question 6:
If a patient has a serious shoulder injury, do you think these views will be helpful?
Likely not, since a patient will be unwilling or unable to move their humerus into internal and external rotation positions if they have a serious injury, such as a fracture or dislocation. In those situations, other special views can be done that do not require the patient to move their arm. We can move the x-ray equipment around to get other angles that can be useful.



Case 2
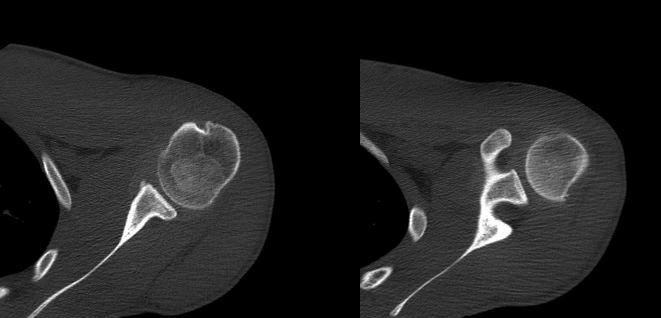
This is a study on a different patient with similar history to our original patient--prior shoulder dislocation, and Hill-Sachs deformity on shoulder radiography.
Question 7:
a) What is this study?
This is a shoulder CT in the axial plane, displayed with bone windows. No IV contrast is present. The humerus is at the patient's side, in neutral position (not anatomic position, which is palms forward, producing external rotation of the humerus).
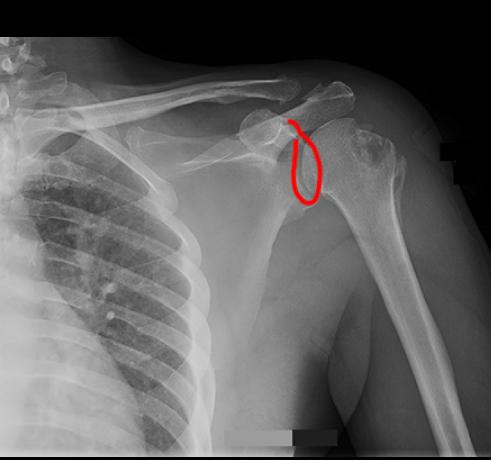
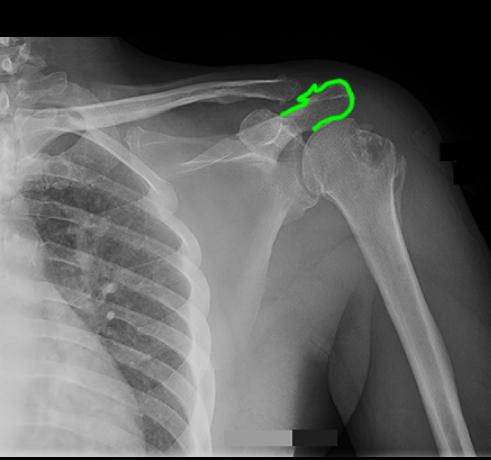
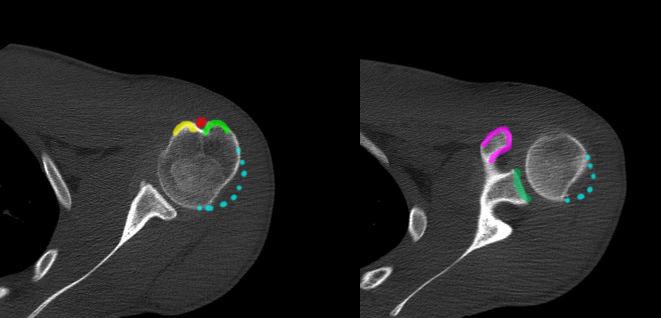
b) What are the outlined structures on the study, shown below?
Red is the position of the biceps tendon, in the intertubercular groove. Yellow is the lesser tubercle of the humerus. Light green indicates the greater tubercle of the humerus. The humeral head is not round, but is dented in laterally. The normal shape of the humerus is shown by the blue dotted line. The coracoid is shown in purple and the glenoid in dark green.
Case 2
This is a different imaging study on another patient with shoulder pain.
Question 8:
What is this study?
This study is called an arthrogram, in this case, a shoulder arthrogram. An arthrogram involves insertion of a needle into a joint space, and injection of radio-opaque contrast material (or gadolinium-based contrast material, if MR is to be done afterwards), to outline the joint space. This also shows the articular cartilage better than can be shown on a regular radiograph. If necessary, a CT can be done following this procedure to get a better 3D idea of how structures are oriented. Arthrograms can be done on virtually any joint, but most commonly are used in the hip, shoulder and knee.
Case 2
This is a young patient with wrist pain.
Question 9:
a) What are is this study?
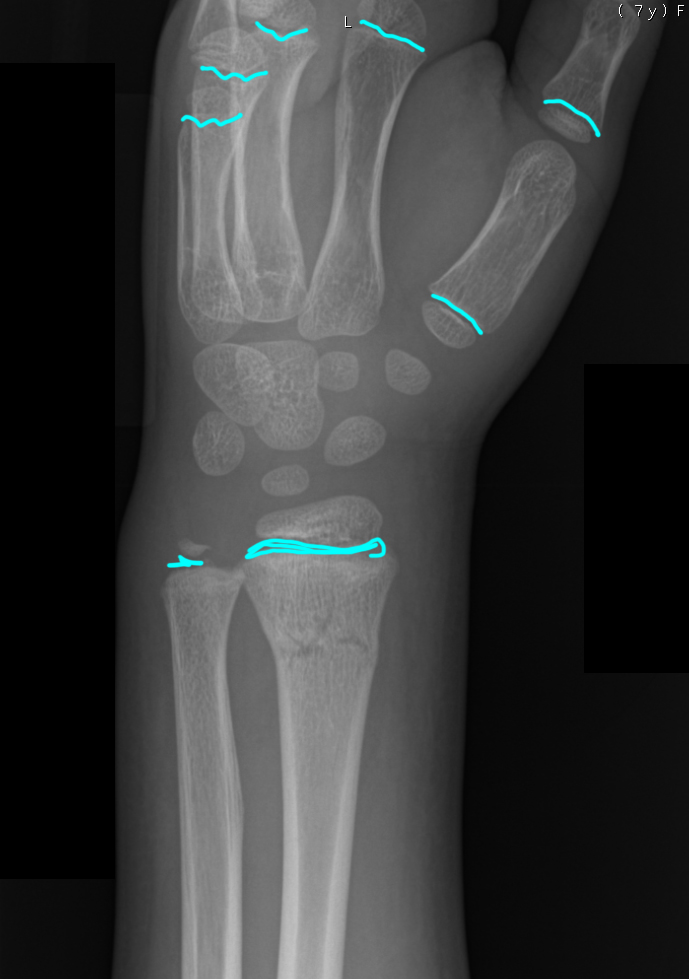
This is a radiograph of the wrist in an oblique projection. Since the hand, foot, wrist and ankle are complicated areas, additional views are often obtained besides just an AP and a lateral view.
b) How can you tell that this is a young patient?
Click on Mystery1 below to see the location of transverse lucent bands in many of the bones of the forearm and hand. These lucent bands are growth plates, made of cartilage. They indicate that the patient is skeletally immature. In fact, if you refer to sets of standardized images of children of different ages, you can use the location, number and appearance of the growth plates to get a very accurate estimate of the patient's age.
c) What is abnormal?
Click on Mystery2 below to see a nondisplaced fracture of the distal radius. It is important not to mistake growth plates for fractures, or to miss fractures thinking that they are growth plates. Fractures are more irregular than growth plates and this lucent band is not at the expected location of a growth plate, which should be located at the junction of metaphysis and epiphysis.